You might also like
- Nurse Practitioner Clinical Protocol: Management of CellulitisDocument11 pagesNurse Practitioner Clinical Protocol: Management of CellulitisJason MarshallNo ratings yet
- Cellulitis Guidelines, CREST, 05 PDFDocument31 pagesCellulitis Guidelines, CREST, 05 PDFanathasia_christineNo ratings yet
- Case Pres CellulitisDocument97 pagesCase Pres CellulitischelybabyjynxNo ratings yet
- Cellulitis of The Lower Limbs: Incidence, Diagnosis and ManagementDocument4 pagesCellulitis of The Lower Limbs: Incidence, Diagnosis and Managementjenifer paathNo ratings yet
- Acute Cellulitis and Erysipelas in Adults - Treatment - UpToDateDocument28 pagesAcute Cellulitis and Erysipelas in Adults - Treatment - UpToDateYahir PerezNo ratings yet
- Cellulitis and Skin AbscessDocument18 pagesCellulitis and Skin AbscessAnonymous ZUaUz1wwNo ratings yet
- Cellulitis Rrapi, R.Document13 pagesCellulitis Rrapi, R.AkasorachiNo ratings yet
- Viewarticle 992915 PrintDocument6 pagesViewarticle 992915 PrintVedat KacarNo ratings yet
- GetpdfDocument17 pagesGetpdfnurulutamimarzaNo ratings yet
- Cellulitis: Current Insights Into Pathophysiology and Clinical ManagementDocument13 pagesCellulitis: Current Insights Into Pathophysiology and Clinical Managementtucto849915No ratings yet
- Acute Cellulitis and Erysipelas in Adults - Treatment - UpToDateDocument34 pagesAcute Cellulitis and Erysipelas in Adults - Treatment - UpToDateBrian VianaNo ratings yet
- Infectious Diseases - 05Document27 pagesInfectious Diseases - 05Arthur YanezNo ratings yet
- Cellulitis: A Review of Pathogenesis, Diagnosis, and ManagementDocument13 pagesCellulitis: A Review of Pathogenesis, Diagnosis, and ManagementSantiago OcampoNo ratings yet
- Combined Cellulitis - FinalDocument78 pagesCombined Cellulitis - Finalsaru_patel0% (1)
- Literature Review CellulitisDocument6 pagesLiterature Review Cellulitisc5qe3qg3100% (1)
- CellulitisDocument5 pagesCellulitisaimigdragonNo ratings yet
- Clinical Approach BlistersDocument25 pagesClinical Approach BlistersIsaacGonzalezNo ratings yet
- Acute Cellulitis and Erysipelas in Adults TreatmentDocument33 pagesAcute Cellulitis and Erysipelas in Adults TreatmentNatália CândidoNo ratings yet
- Skin PiksDocument7 pagesSkin PiksMavra zNo ratings yet
- Causes and Management of Cellulitis: PathologyDocument4 pagesCauses and Management of Cellulitis: PathologyIsmail YusufNo ratings yet
- Eritema Elevatum DiutinunDocument8 pagesEritema Elevatum DiutinunVar AndaNo ratings yet
- CCJM Distinguishing Cellulitis From Its MimicsDocument6 pagesCCJM Distinguishing Cellulitis From Its MimicsBrian HarrisNo ratings yet
- Furuncles and Carbuncles: CellulitisDocument9 pagesFuruncles and Carbuncles: CellulitissanjivdasNo ratings yet
- Cellulitis and Erysipelas in Adults - Treatment - UpToDateDocument39 pagesCellulitis and Erysipelas in Adults - Treatment - UpToDateJuan Sebastian SalinasNo ratings yet
- Common Bacterial Skin InfectionsDocument6 pagesCommon Bacterial Skin InfectionsagusNo ratings yet
- Cellulitis: Clinical PracticeDocument9 pagesCellulitis: Clinical PracticeBobby S PromondoNo ratings yet
- CellulitisDocument3 pagesCellulitisAllen MallariNo ratings yet
- Celulitis PDFDocument9 pagesCelulitis PDFGazade GarciaNo ratings yet
- CELLULITISSSDocument5 pagesCELLULITISSSLet BorlagdanNo ratings yet
- Cellulitis and Skin Abscess in Adults - Treatment - UpToDateDocument16 pagesCellulitis and Skin Abscess in Adults - Treatment - UpToDateIsabella Gutierrez CarabaliNo ratings yet
- Benedictmitnick2019 PDFDocument9 pagesBenedictmitnick2019 PDFArthur TeixeiraNo ratings yet
- Seminar On Spread of Oral Infections: Presented By:-Dr. Ipsha DhaliDocument97 pagesSeminar On Spread of Oral Infections: Presented By:-Dr. Ipsha DhaliDua'a Ma'anNo ratings yet
- An Update On The Treatment and Management of Cellulitis: Practical DermatologyDocument7 pagesAn Update On The Treatment and Management of Cellulitis: Practical DermatologyIndra RukmanaNo ratings yet
- Oral Versus Parenteral TherapyDocument7 pagesOral Versus Parenteral TherapymanuelNo ratings yet
- Diganosa RashDocument12 pagesDiganosa RashChoirul WizaNo ratings yet
- Study of Clinical Profile of Acute Limb Cellulitis Patients in Tertiary Care CenterDocument7 pagesStudy of Clinical Profile of Acute Limb Cellulitis Patients in Tertiary Care CenterOmkar ShendeNo ratings yet
- Group2-Vasculitis-Sec7-2 2Document7 pagesGroup2-Vasculitis-Sec7-2 2c.caeNo ratings yet
- SelulitisDocument5 pagesSelulitisdnswrNo ratings yet
- Cellulitis: The Right Clinical Information, Right Where It's NeededDocument59 pagesCellulitis: The Right Clinical Information, Right Where It's NeededJohnnyDEroNo ratings yet
- Makalah SelulitisDocument26 pagesMakalah Selulitisdr WiyogoNo ratings yet
- Risk, Prevention, Diagnosis, and Management of Cellulitis and ErysipelasDocument10 pagesRisk, Prevention, Diagnosis, and Management of Cellulitis and ErysipelasHanunNo ratings yet
- Manifestaciones Dermatologicas en MI PDFDocument24 pagesManifestaciones Dermatologicas en MI PDFDiego ValadezNo ratings yet
- Selulitis: Backround: Skin Diseases Caused by Staphylococcus, Streptococcus, or by Both CalledDocument10 pagesSelulitis: Backround: Skin Diseases Caused by Staphylococcus, Streptococcus, or by Both CalledAgung HNo ratings yet
- Clinical Pearls DermatologíamatologyDocument4 pagesClinical Pearls DermatologíamatologyMaritza24No ratings yet
- Biology Investigatory ProjectDocument16 pagesBiology Investigatory ProjectpreranaNo ratings yet
- CASE STUDY 2011-CellulitisDocument34 pagesCASE STUDY 2011-Cellulitiscyrilcarinan75% (4)
- Stasis Dermatitis: An Overview of Its Clinical Presentation, Pathogenesis, and ManagementDocument12 pagesStasis Dermatitis: An Overview of Its Clinical Presentation, Pathogenesis, and ManagementNydia OngaliaNo ratings yet
- WO No.10 Week 2Document4 pagesWO No.10 Week 2ReginaJacobNo ratings yet
- BR J Dermatol - 2022 - Dissemond - Inflammatory Skin Diseases and WoundsDocument11 pagesBR J Dermatol - 2022 - Dissemond - Inflammatory Skin Diseases and Woundsวสุชล ชัยชาญNo ratings yet
- Cellulitis - Biology Science Fair Project IdeasDocument4 pagesCellulitis - Biology Science Fair Project IdeasEPFO AKURDINo ratings yet
- ABC of Wound Healing WWW - Dof3tna - Net WWW - Egydr.com Drhamdy2009Document49 pagesABC of Wound Healing WWW - Dof3tna - Net WWW - Egydr.com Drhamdy2009steadiNo ratings yet
- Jurnal KulitDocument25 pagesJurnal Kulitwulandari putriNo ratings yet
- CellulitisDocument8 pagesCellulitisTricia Llorin100% (1)
- Michelet T I 2020Document5 pagesMichelet T I 2020Daniela RotaruNo ratings yet
- Large and Medium Size Vessel and Single Organ VasculitisFrom EverandLarge and Medium Size Vessel and Single Organ VasculitisCarlo SalvaraniNo ratings yet
- Surviving Leukemia and Hodgkin's Lymphoma: An Overview Of Effective Treatment MethodsFrom EverandSurviving Leukemia and Hodgkin's Lymphoma: An Overview Of Effective Treatment MethodsNo ratings yet
- NIH Public Access: Author ManuscriptDocument20 pagesNIH Public Access: Author ManuscriptJason MarshallNo ratings yet
- Yun Li and Jing Zheng: Taylor & Francis Inc. ISSN: 1062-3329 Print/1029-2373 Online DOI: 10.1080/10623320590933743Document20 pagesYun Li and Jing Zheng: Taylor & Francis Inc. ISSN: 1062-3329 Print/1029-2373 Online DOI: 10.1080/10623320590933743Jason MarshallNo ratings yet
- Cellulitis and Wound Management: Joanne Martin, RN, BSN, CWOCN Deaconess Home Health Care, Savannah, TNDocument1 pageCellulitis and Wound Management: Joanne Martin, RN, BSN, CWOCN Deaconess Home Health Care, Savannah, TNJason MarshallNo ratings yet
- Research Article: Effects of Three Types of Japanese Honey On Full-Thickness Wound in MiceDocument11 pagesResearch Article: Effects of Three Types of Japanese Honey On Full-Thickness Wound in MiceJason MarshallNo ratings yet
- Nurse Practitioner Clinical Protocol: Management of CellulitisDocument11 pagesNurse Practitioner Clinical Protocol: Management of CellulitisJason MarshallNo ratings yet
- Report Documentation Page: Headquarters Information Please Do Return Your To The Above AddressDocument6 pagesReport Documentation Page: Headquarters Information Please Do Return Your To The Above AddressJason MarshallNo ratings yet
- Fibrin Cuff Lysis in Chronic Venous Ulcfrs TreatedDocument4 pagesFibrin Cuff Lysis in Chronic Venous Ulcfrs TreatedJason MarshallNo ratings yet
- 1 Fluid and ElectrolyteDocument51 pages1 Fluid and ElectrolyteSanjiv SharmaNo ratings yet
- 2nd Reporters 119Document9 pages2nd Reporters 119Ellen Joyce FlorNo ratings yet
- Management of Hospital PharmacyDocument33 pagesManagement of Hospital PharmacyZainab JavaidNo ratings yet
- HBV Easl-CpgDocument48 pagesHBV Easl-CpgAqila MumtazNo ratings yet
- Mindfulness in Schools - Promoting Social and Emotional Learning IDocument34 pagesMindfulness in Schools - Promoting Social and Emotional Learning ILola Ouroburos0% (1)
- Alergy 2Document2 pagesAlergy 2Wiwiek Anindita AfrilyantariNo ratings yet
- Lung Cancer Case Study NihDocument4 pagesLung Cancer Case Study NihMarc FosterNo ratings yet
- The Beck Depression Inventory: The Pharma Innovation - JournalDocument7 pagesThe Beck Depression Inventory: The Pharma Innovation - JournaldevNo ratings yet
- Dr. C.T. Karthikeyan, Associate Professor, Dept. of General SurgeryDocument40 pagesDr. C.T. Karthikeyan, Associate Professor, Dept. of General SurgeryNaveen RajeshwarNo ratings yet
- Schizophrenic Brains Not Fooled by Optical Illusion WIREDDocument3 pagesSchizophrenic Brains Not Fooled by Optical Illusion WIREDJeffPitnerNo ratings yet
- Clinical Review: Acute CholecystitisDocument5 pagesClinical Review: Acute CholecystitisElsa SimangunsongNo ratings yet
- Gordon's Pattern of FunctDocument2 pagesGordon's Pattern of FunctPau ManalangNo ratings yet
- Medical ReportDocument5 pagesMedical ReportRuthdel KazumiNo ratings yet
- Puerperal SepsisDocument4 pagesPuerperal SepsisSonali NayakNo ratings yet
- Jurnal Cardiac ArrestDocument10 pagesJurnal Cardiac ArrestAhmad NurdinNo ratings yet
- Physio of PhonationDocument71 pagesPhysio of PhonationRamya CherukuriNo ratings yet
- LAMPE Harald Ignatius HubertusDocument100 pagesLAMPE Harald Ignatius HubertusSumaya NoorNo ratings yet
- 1968 Long-Term Total Parenteral Nutrition With Growth, Development, and Positive Nitrogen Balance. SURGERYDocument4 pages1968 Long-Term Total Parenteral Nutrition With Growth, Development, and Positive Nitrogen Balance. SURGERYChristine ChambersNo ratings yet
- Grand Case Presentation InformationDocument7 pagesGrand Case Presentation InformationCristina L. JaysonNo ratings yet
- Ward ClassDocument7 pagesWard ClassAYESSA JOELLE FOMOKAONo ratings yet
- WWW KFSHRC Edu SaDocument3 pagesWWW KFSHRC Edu Sawaqas_xsNo ratings yet
- NHPPD Calculating StaffingDocument3 pagesNHPPD Calculating Staffingodin9360343No ratings yet
- OB PACU Severe PreeclampsiaDocument65 pagesOB PACU Severe Preeclampsiasurbakti_christineNo ratings yet
- Print CouponDocument1 pagePrint CouponHEATHER BNo ratings yet
- Intervention Session TemplateDocument4 pagesIntervention Session Templateapi-580038681No ratings yet
- Hematopoietic Stem Cell Transplantation For Thalassemia: Javid Gaziev and Guido LucarelliDocument14 pagesHematopoietic Stem Cell Transplantation For Thalassemia: Javid Gaziev and Guido LucarelliRatna AzizahNo ratings yet
- Drug Provocation Test, Tes Provokasi ObatDocument12 pagesDrug Provocation Test, Tes Provokasi ObatKertiasihwayanNo ratings yet
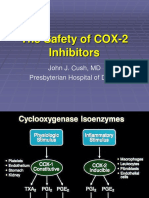
- The Safety of COX-2 Inhibitors: John J. Cush, MD Presbyterian Hospital of DallasDocument29 pagesThe Safety of COX-2 Inhibitors: John J. Cush, MD Presbyterian Hospital of DallasHerry HendrayadiNo ratings yet
- General AnaesthesiaDocument99 pagesGeneral Anaesthesiamcshah19No ratings yet
- Psych NSG Sample QuestionsDocument7 pagesPsych NSG Sample Questionspaul100% (9)