You might also like
- Reconstruction of Defects of The Posterior Pinna.15Document4 pagesReconstruction of Defects of The Posterior Pinna.15cliffwinskyNo ratings yet
- Semilunar Coronally Repositioned FlapDocument5 pagesSemilunar Coronally Repositioned FlapTarun Kumar Bhatnagar100% (1)
- Basic Brain Anatomy and Physiology PDFDocument10 pagesBasic Brain Anatomy and Physiology PDFSenthilkumar Thiyagarajan100% (3)
- McKenzie Self-Treatments For SciaticaDocument3 pagesMcKenzie Self-Treatments For SciaticaSenthilkumar Thiyagarajan80% (5)
- Orthopedic Assessment For PhysiotherapistDocument3 pagesOrthopedic Assessment For Physiotherapistsenthilkumar76% (21)
- Varaha KavachamDocument10 pagesVaraha KavachamMukunda VenugopalNo ratings yet
- Surgical IncisionsDocument35 pagesSurgical IncisionsRoselle Angela Valdoz MamuyacNo ratings yet
- Surgical Incisions AbdomenDocument9 pagesSurgical Incisions Abdomensnapb202No ratings yet
- Sites of IncisionDocument11 pagesSites of IncisionMi LaNo ratings yet
- Me and DR KhalidDocument29 pagesMe and DR KhalidUmer KhanNo ratings yet
- Surgical Incisions: STJ - Dr. Aylin Mert 0902110019Document22 pagesSurgical Incisions: STJ - Dr. Aylin Mert 0902110019NiyaNo ratings yet
- Incision SitesDocument4 pagesIncision SitesmidskiescreamzNo ratings yet
- Classification of IncisionsDocument7 pagesClassification of IncisionsEleazar MagsinoNo ratings yet
- Tibial Pilon Fractures - OrIF and or External FixationDocument9 pagesTibial Pilon Fractures - OrIF and or External FixationsteoeviciNo ratings yet
- The Keystone Design Perforator Island Flap in Reconstructive SurgeryDocument9 pagesThe Keystone Design Perforator Island Flap in Reconstructive SurgeryCristina Iulia100% (1)
- Surgicalincisions 150519180458 Lva1 App6892 PDFDocument22 pagesSurgicalincisions 150519180458 Lva1 App6892 PDFAbdul Qadir KhurramNo ratings yet
- Print Test Page556Document5 pagesPrint Test Page556andhikaaji4980No ratings yet
- UELI EGLI, WERNER H. VOLLMER AND KLAUS H. RATEITSCHAK. Follow-Up Studies of Free Gingival GraftsDocument8 pagesUELI EGLI, WERNER H. VOLLMER AND KLAUS H. RATEITSCHAK. Follow-Up Studies of Free Gingival GraftsSebastián BernalNo ratings yet
- Tibial Fractures Useful Plastering Technique: MethodDocument4 pagesTibial Fractures Useful Plastering Technique: MethodgregraynerNo ratings yet
- Kugel Repair For HerniasDocument21 pagesKugel Repair For HerniasElias Emmanuel JaimeNo ratings yet
- Articol RamirezDocument6 pagesArticol RamirezDragoș PopaNo ratings yet
- Skin IncisionsDocument1 pageSkin IncisionsShanna Marie MelodiaNo ratings yet
- Review Article: A History of Endoscopic Lumbar Spine Surgery: What Have We Learnt?Document9 pagesReview Article: A History of Endoscopic Lumbar Spine Surgery: What Have We Learnt?cogajoNo ratings yet
- Interstitial Incisional Hernia Following Appendectomy: Case ReportDocument2 pagesInterstitial Incisional Hernia Following Appendectomy: Case ReportSCJUBv Chirurgie INo ratings yet
- Jurnal OrthopediDocument9 pagesJurnal OrthopediRetti TriNo ratings yet
- Scitemed Imj 2017 00036-1Document4 pagesScitemed Imj 2017 00036-1bernicemerryNo ratings yet
- TECNICADocument7 pagesTECNICASiris Rieder GarridoNo ratings yet
- Review Article: Abdominal Incisions in General Surgery: A ReviewDocument5 pagesReview Article: Abdominal Incisions in General Surgery: A ReviewMoxa ShahNo ratings yet
- Generations of The Plug-and-Patch Repair: Its Development and Lessons From HistoryDocument1 pageGenerations of The Plug-and-Patch Repair: Its Development and Lessons From HistorycesaliapNo ratings yet
- Insisi LukaDocument48 pagesInsisi LukaRiska RiantiNo ratings yet
- Hernia Repair 3Document38 pagesHernia Repair 3caliptra36No ratings yet
- Rosenbrg-Goss2020 Article AModifiedTechniqueOfTemporomanDocument10 pagesRosenbrg-Goss2020 Article AModifiedTechniqueOfTemporomanMarcela RibeiroNo ratings yet
- Keystone Flap: Kyle S. Ettinger, MD, DDS, Rui P. Fernandes, MD, DMD, FRCS (Ed), Kevin Arce, MD, DMDDocument14 pagesKeystone Flap: Kyle S. Ettinger, MD, DDS, Rui P. Fernandes, MD, DMD, FRCS (Ed), Kevin Arce, MD, DMDlaljadeff12No ratings yet
- Marinelli - Surgical Approaches - 2014Document9 pagesMarinelli - Surgical Approaches - 2014Giulio PriftiNo ratings yet
- Pedicled Fasciocutaneous and Adipofascial FlapsDocument16 pagesPedicled Fasciocutaneous and Adipofascial FlapspuchioNo ratings yet
- Notes Made Easy TraumaDocument74 pagesNotes Made Easy TraumaMorshed Mahbub AbirNo ratings yet
- Incisional Hernia Open ProceduresDocument25 pagesIncisional Hernia Open ProceduresElias Emmanuel JaimeNo ratings yet
- Common Surgical IncisionsDocument17 pagesCommon Surgical IncisionsShaika-Riza SakironNo ratings yet
- Incisional HerniaDocument13 pagesIncisional HerniaMaya Dewi permatasariNo ratings yet
- Management of Complex Orbital Fractures: Article in PressDocument5 pagesManagement of Complex Orbital Fractures: Article in Pressstoia_sebiNo ratings yet
- Transition To Anterior Approach in Primary Total Hip Arthroplasty Learning Curve ComplicationsDocument7 pagesTransition To Anterior Approach in Primary Total Hip Arthroplasty Learning Curve ComplicationsAthenaeum Scientific PublishersNo ratings yet
- Orbitotomi MedscapeDocument9 pagesOrbitotomi MedscapeBonita AsyigahNo ratings yet
- Abdominal Trauma Lecture SurgeryDocument9 pagesAbdominal Trauma Lecture Surgerylarzy.larasumibcay27No ratings yet
- Kyestone Flaps PDFDocument9 pagesKyestone Flaps PDFDra. Bianca Ariza MoralesNo ratings yet
- El-Sayyad - Management of Burst Abdomen and Abdominal Wall ReconstructionDocument10 pagesEl-Sayyad - Management of Burst Abdomen and Abdominal Wall Reconstructionrhyzik reeNo ratings yet
- UntitledDocument35 pagesUntitledGiselmar Soto DíazNo ratings yet
- Soft Tissue Management in Implant DentistryDocument37 pagesSoft Tissue Management in Implant DentistryAhmad AlhakimNo ratings yet
- Eaat 04 I 1 P 19Document4 pagesEaat 04 I 1 P 19allthewayhomeNo ratings yet
- Facial Fractures I Upper Two ThirdsDocument35 pagesFacial Fractures I Upper Two ThirdsJulia Recalde Reyes100% (1)
- The Palatal Advanced Flap: A Pedicle Flap For Primary Coverage of Immediately Placed ImplantsDocument7 pagesThe Palatal Advanced Flap: A Pedicle Flap For Primary Coverage of Immediately Placed ImplantsMárcia ChatelieNo ratings yet
- Endoskopik 2.brankialDocument5 pagesEndoskopik 2.brankialDogukan DemirNo ratings yet
- Akira Saito Et Al. (2009)Document4 pagesAkira Saito Et Al. (2009)Janardana GedeNo ratings yet
- Arthroplasty TodayDocument7 pagesArthroplasty TodaySanty OktavianiNo ratings yet
- LWBK836 Ch98 p1021-1030Document10 pagesLWBK836 Ch98 p1021-1030metasoniko81No ratings yet
- Jum 15608Document5 pagesJum 15608nessim zouariNo ratings yet
- J Neurosurg Case Lessons Article CASE2190Document4 pagesJ Neurosurg Case Lessons Article CASE2190chaiimaefrNo ratings yet
- Hindquarter IJOCDocument4 pagesHindquarter IJOCRyanAdnaniNo ratings yet
- Rib FractureDocument6 pagesRib FracturenasyilaputriNo ratings yet
- Clinical Maxillary Sinus Elevation SurgeryFrom EverandClinical Maxillary Sinus Elevation SurgeryDaniel W. K. KaoNo ratings yet
- The Ileoanal Pouch: A Practical Guide for Surgery, Management and TroubleshootingFrom EverandThe Ileoanal Pouch: A Practical Guide for Surgery, Management and TroubleshootingJanindra WarusavitarneNo ratings yet
- The MeniscusFrom EverandThe MeniscusPhilippe BeaufilsNo ratings yet
- Current Techniques in Canine and Feline NeurosurgeryFrom EverandCurrent Techniques in Canine and Feline NeurosurgeryAndy ShoresNo ratings yet
- A Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersFrom EverandA Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersNo ratings yet
- Ankle TappingDocument4 pagesAnkle TappingSenthilkumar ThiyagarajanNo ratings yet
- Abdominal Stretching ExsDocument1 pageAbdominal Stretching ExsSenthilkumar ThiyagarajanNo ratings yet
- Active Cycle Breathing Technique-Easy DemoDocument3 pagesActive Cycle Breathing Technique-Easy DemoSenthilkumar ThiyagarajanNo ratings yet
- Cervical ExerciseDocument1 pageCervical ExerciseSenthilkumar Thiyagarajan100% (1)
- Aids To The Examination of Peripheral Nervous SystemDocument67 pagesAids To The Examination of Peripheral Nervous SystemSenthilkumar ThiyagarajanNo ratings yet
- Anatomymnemonics PDFDocument28 pagesAnatomymnemonics PDFSenthilkumar ThiyagarajanNo ratings yet
- Postromedial Dic ProlapsDocument3 pagesPostromedial Dic ProlapsSenthilkumar Thiyagarajan100% (1)
- C:/Documents and Settings/student/Desktop/physiotherapy Protocol FOR HEMIPLEGIC PDFDocument13 pagesC:/Documents and Settings/student/Desktop/physiotherapy Protocol FOR HEMIPLEGIC PDFSenthilkumar ThiyagarajanNo ratings yet
- Above Knee Amputation Good One PDFDocument9 pagesAbove Knee Amputation Good One PDFSenthilkumar Thiyagarajan100% (1)
- Post Natal Exercise PrescriptionDocument8 pagesPost Natal Exercise PrescriptionSenthilkumar ThiyagarajanNo ratings yet
- Above Knee Amputation Exc PDFDocument5 pagesAbove Knee Amputation Exc PDFSenthilkumar ThiyagarajanNo ratings yet
- All Orthopedic TestsDocument7 pagesAll Orthopedic Testschandran2679No ratings yet
- Foxlite 2.0 Manual: Foxsupport@Geneko - RsDocument50 pagesFoxlite 2.0 Manual: Foxsupport@Geneko - RsFoxLiteNo ratings yet
- Rujukan OshaDocument22 pagesRujukan Oshahakim999No ratings yet
- Comparison of Horizontal Lip Pressure - R0Document2 pagesComparison of Horizontal Lip Pressure - R0AndiNo ratings yet
- IES MdijDocument5 pagesIES MdijAnonymous fFsGiyNo ratings yet
- Pinyin+character Stroke OrderDocument4 pagesPinyin+character Stroke OrderAlexandra SmlNo ratings yet
- Non-Destructive Testing For Non-Ferrous Materials Like Aluminium and Copper.Document9 pagesNon-Destructive Testing For Non-Ferrous Materials Like Aluminium and Copper.Raushan JhaNo ratings yet
- Daily Lesson Plan DLP F1 3 - 1Document1 pageDaily Lesson Plan DLP F1 3 - 1chezdinNo ratings yet
- Grammar - Unit 2 - in ClassDocument7 pagesGrammar - Unit 2 - in ClassJhomer Briceño EulogioNo ratings yet
- Peaktronics: Digital High-Resolution ControllerDocument12 pagesPeaktronics: Digital High-Resolution Controllerschmal1975No ratings yet
- (T), (D) or (Id) ? - "-Ed" Past Tense - English PronunciationDocument3 pages(T), (D) or (Id) ? - "-Ed" Past Tense - English PronunciationClaudioNo ratings yet
- Iae1 QPDocument3 pagesIae1 QPyaboyNo ratings yet
- History of Indian AdvertisingDocument13 pagesHistory of Indian AdvertisingdheepaNo ratings yet
- Albert Einstein Background and Early LifeDocument8 pagesAlbert Einstein Background and Early LifeMuhd HafizNo ratings yet
- Cha 2Document5 pagesCha 2ShammimBegumNo ratings yet
- Contemporary World Finals NotesDocument4 pagesContemporary World Finals Notesangelo subaNo ratings yet
- ACCO 101 Partnership Formation For Practice SolvingDocument2 pagesACCO 101 Partnership Formation For Practice SolvingFionna Rei DeGaliciaNo ratings yet
- Huawei eLTE Multimedia Critical Communication System Solution 高清印刷版 (刷新)Document8 pagesHuawei eLTE Multimedia Critical Communication System Solution 高清印刷版 (刷新)Alejandro RojasNo ratings yet
- Cepa-2012-Practice-Exam-Version-A AnswersDocument19 pagesCepa-2012-Practice-Exam-Version-A AnswersGeo KemoNo ratings yet
- Aspirin SynthesisDocument13 pagesAspirin SynthesisJM DreuNo ratings yet
- Post Test Bahasa InggrisDocument8 pagesPost Test Bahasa InggrisristyNo ratings yet
- ZKBiolock Hotel Lock System User Manual V2.0Document89 pagesZKBiolock Hotel Lock System User Manual V2.0Nicolae OgorodnicNo ratings yet
- Laboratory Exercise 1 Matlab Introducction: Name SectionDocument7 pagesLaboratory Exercise 1 Matlab Introducction: Name SectionDean16031997No ratings yet
- 501/423 Cable Gland Type: Flameproof and Increased SafetyDocument1 page501/423 Cable Gland Type: Flameproof and Increased Safetymadhan rajNo ratings yet
- Advanced Power Electronic Functionality For Renewable Energy Integration With The Power GridDocument17 pagesAdvanced Power Electronic Functionality For Renewable Energy Integration With The Power GridtomsiriNo ratings yet
- Igneous RockDocument9 pagesIgneous Rockdeboline mitraNo ratings yet
- Terberg Benschop Yt182 222 Yard Tractor BC 182 Body Carrier Electrical Wiring DiagramDocument22 pagesTerberg Benschop Yt182 222 Yard Tractor BC 182 Body Carrier Electrical Wiring Diagramkathleenterry260595mjz97% (31)
- The Return From One Investment Is 0.711 More Than The Other (Your Answer Is Incorrect)Document6 pagesThe Return From One Investment Is 0.711 More Than The Other (Your Answer Is Incorrect)Dolly TrivediNo ratings yet
- About Myself: - StrenghtsDocument2 pagesAbout Myself: - StrenghtsGabriela MoNo ratings yet
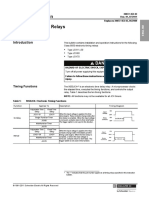
- Instruction Bulletin Electronic Timing Relays: Class 9050 Type JCKDocument4 pagesInstruction Bulletin Electronic Timing Relays: Class 9050 Type JCKKamran IbadovNo ratings yet