You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (347)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- ghq-28 FORMDocument2 pagesghq-28 FORMombo40% (5)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 2021 Abstract Book FINAL - KNC - 040621Document115 pages2021 Abstract Book FINAL - KNC - 040621purplelydiaNo ratings yet
- Practice Test Pediatric Nursing 100 ItemsDocument17 pagesPractice Test Pediatric Nursing 100 ItemsMichelle Lureineil Dajao100% (3)
- Herbs-Sam CoffmanDocument9 pagesHerbs-Sam CoffmanSilambarasu Karuppiah0% (1)
- Ggi12193 PDF Jsessionid f01t02Document9 pagesGgi12193 PDF Jsessionid f01t02omboNo ratings yet
- 6 Minute Walk Test InstructionsDocument3 pages6 Minute Walk Test InstructionsJill LoveNo ratings yet
- Suck Training PDFDocument2 pagesSuck Training PDFomboNo ratings yet
- Denis ClassificationDocument2 pagesDenis ClassificationomboNo ratings yet
- Alternative FeedingDocument4 pagesAlternative FeedingomboNo ratings yet
- Case AnalysisDocument1 pageCase AnalysisomboNo ratings yet
- Expected Outcomes: What You Should Know: T1-9 Spinal Cord InjuryDocument23 pagesExpected Outcomes: What You Should Know: T1-9 Spinal Cord InjuryomboNo ratings yet
- Richi HW Neurodiv PMR Dept.Document5 pagesRichi HW Neurodiv PMR Dept.omboNo ratings yet
- Case Report: MR - NC, 21 Y.o, Right Handed, Lives in Pasanggrahan Street Cisalak Subang, Reffered FromDocument8 pagesCase Report: MR - NC, 21 Y.o, Right Handed, Lives in Pasanggrahan Street Cisalak Subang, Reffered FromomboNo ratings yet
- WPC 096853Document7 pagesWPC 096853omboNo ratings yet
- 24 - Liquor AnaliseDocument6 pages24 - Liquor AnaliseomboNo ratings yet
- Chapter 7 Examination of Cerebrospinal Fluid and Serous Membrane FluidDocument8 pagesChapter 7 Examination of Cerebrospinal Fluid and Serous Membrane FluidomboNo ratings yet
- Physiology of Pain: Guide To Pain Management in Low-Resource SettingsDocument6 pagesPhysiology of Pain: Guide To Pain Management in Low-Resource SettingsomboNo ratings yet
- Soal Ujian Semester 1 DMDocument10 pagesSoal Ujian Semester 1 DMomboNo ratings yet
- Constipation Biofeedback For Pelvic Floor Dysfunction In: Data Supplement ReferencesDocument5 pagesConstipation Biofeedback For Pelvic Floor Dysfunction In: Data Supplement ReferencesomboNo ratings yet
- Myomed932 The RoleDocument8 pagesMyomed932 The RoleomboNo ratings yet
- Tadic S, Schaefer W, Griffiths D, Resnick N 1. University of PittsburghDocument2 pagesTadic S, Schaefer W, Griffiths D, Resnick N 1. University of PittsburghomboNo ratings yet
- VCUG (Voiding Cystourethrogram) What It IsDocument3 pagesVCUG (Voiding Cystourethrogram) What It IsNinaNo ratings yet
- Urinary RetentionDocument6 pagesUrinary Retentionjakenathanielvelasco50% (2)
- DiGeorge SyndromeDocument11 pagesDiGeorge SyndromeRupesh MohandasNo ratings yet
- Trafficking of Women HarshitaDocument31 pagesTrafficking of Women HarshitaRajkumar SinghalNo ratings yet
- Urinary and Male GenitalDocument116 pagesUrinary and Male GenitalMultazam ZamNo ratings yet
- National Antibiotic Pedia GuidelinesDocument149 pagesNational Antibiotic Pedia GuidelinesGg GreyNo ratings yet
- BRT Surgery - Urology Part 2Document3 pagesBRT Surgery - Urology Part 2Princess Sittie Asiah AbdullahNo ratings yet
- UTI Practicum Make-Up Assignment FINALDocument8 pagesUTI Practicum Make-Up Assignment FINALlmstar98No ratings yet
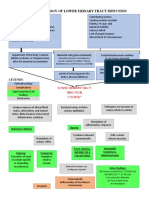
- Pathophysiology of Lower Urinary Tract InfectionDocument1 pagePathophysiology of Lower Urinary Tract InfectionSTORAGE FILENo ratings yet
- Coc 2022 Reviewed Q & ADocument74 pagesCoc 2022 Reviewed Q & ASneeze LouderNo ratings yet
- Bakteriologi Urin 2020Document23 pagesBakteriologi Urin 2020QUINITA NORONHANo ratings yet
- Pathology of The Male GUTDocument108 pagesPathology of The Male GUTHoque Mohammed Newaz ShorifulNo ratings yet
- Aafp Uti GuidelinesDocument10 pagesAafp Uti GuidelinesCess Lagera YbanezNo ratings yet
- Protocol Book For OBGYNDocument41 pagesProtocol Book For OBGYNShabir BadakhshNo ratings yet
- Homeo-11 RrUBRICSDocument32 pagesHomeo-11 RrUBRICSRashid MahmoodNo ratings yet
- S.C. Madan Homeopathy Cures Where Allopathy Fails: LeseprobeDocument6 pagesS.C. Madan Homeopathy Cures Where Allopathy Fails: LeseprobeTanuj TyagiNo ratings yet
- Alaska Tribal Health Webinar Series Dr. Emily Hogeland Pediatric Hospitalist Alaska Native Medical Center September 3, 2021Document36 pagesAlaska Tribal Health Webinar Series Dr. Emily Hogeland Pediatric Hospitalist Alaska Native Medical Center September 3, 2021solthneNo ratings yet
- Monuril Vs CiproDocument7 pagesMonuril Vs Ciproalaa morsyNo ratings yet
- RenalDocument60 pagesRenalEdmalyn Dela CruzNo ratings yet
- CHCCCS011 Student Assessment Theory Task 06122020 - Ha NguyenDocument29 pagesCHCCCS011 Student Assessment Theory Task 06122020 - Ha NguyenNguyen Ha0% (1)
- DR Jones Cat Health Web Clinic Slides 1222Document222 pagesDR Jones Cat Health Web Clinic Slides 1222Haider Al Zamily100% (1)
- Approach To HematuriaDocument15 pagesApproach To HematuriaArsalan NadeemNo ratings yet
- ACKD Susp Lupus NefritisDocument61 pagesACKD Susp Lupus Nefritisrastu karyanaNo ratings yet
- 2022 December BlueprintDocument38 pages2022 December BlueprintNonoy JoyaNo ratings yet
- Family Case Study - BN4A Group 2Document46 pagesFamily Case Study - BN4A Group 2Rene John Francisco100% (1)
- HLB, NME, M& M OSCE Notes - University of Manchester, WL GanDocument45 pagesHLB, NME, M& M OSCE Notes - University of Manchester, WL GanWeh Loong Gan100% (2)
- Utrine ProlapseDocument22 pagesUtrine ProlapseMuskan RastogiNo ratings yet