You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Thomas R. Quackenbush - Relearning To See Improve Your Eyesight Naturally! PDFDocument514 pagesThomas R. Quackenbush - Relearning To See Improve Your Eyesight Naturally! PDFtyrant250100% (3)
- v1.0 Endgültig 15242409Document2 pagesv1.0 Endgültig 15242409Iqbal RahmansyahNo ratings yet
- CincinnatiDocument1 pageCincinnatiIqbal RahmansyahNo ratings yet
- Recent Decline in Births in The United States, 2007-2009: NCHS Data Brief No. 60 March 2011Document8 pagesRecent Decline in Births in The United States, 2007-2009: NCHS Data Brief No. 60 March 2011Iqbal RahmansyahNo ratings yet
- Did You Know? Symptoms Managing Depression: Quick Depression Assessment: Patient Health Questionnaire-9 (PHQ-9)Document2 pagesDid You Know? Symptoms Managing Depression: Quick Depression Assessment: Patient Health Questionnaire-9 (PHQ-9)Iqbal RahmansyahNo ratings yet
- Interstitial Lung Disease Guideline Appendix 2 Drug Induced ILD: Classification With ExamplesDocument1 pageInterstitial Lung Disease Guideline Appendix 2 Drug Induced ILD: Classification With ExamplesIqbal RahmansyahNo ratings yet
- Book Reviews: Nutrigenetics and Nutrigenomics. World Review of Nutrition and Dietetics, Volume 93, 2004. EditorsDocument1 pageBook Reviews: Nutrigenetics and Nutrigenomics. World Review of Nutrition and Dietetics, Volume 93, 2004. EditorsIqbal RahmansyahNo ratings yet
- Molecular Mechanisms of The Effects of Ionizing Radiation: Free Radicals From DNA and Model CompoundsDocument2 pagesMolecular Mechanisms of The Effects of Ionizing Radiation: Free Radicals From DNA and Model CompoundsIqbal RahmansyahNo ratings yet
- Annex 2: © World Health Organization WHO Technical Report Series, No. 926, 2004Document25 pagesAnnex 2: © World Health Organization WHO Technical Report Series, No. 926, 2004Iqbal RahmansyahNo ratings yet
- Autonomic Drugs 2020 Part 1 IntroDocument29 pagesAutonomic Drugs 2020 Part 1 Introعون عليNo ratings yet
- Muscular SystemDocument49 pagesMuscular SystemHindrix Mitch100% (1)
- Dolphin RelaxationDocument5 pagesDolphin RelaxationThe Healing ToolsNo ratings yet
- Traditional Medicinal Plants in VisayasDocument7 pagesTraditional Medicinal Plants in VisayasErhiecka BasaNo ratings yet
- Genetic MutationDocument27 pagesGenetic MutationKathleen JOy BiasUraNo ratings yet
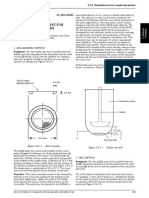
- 2 9 4 Dissolution Test For Transdermal PatchesDocument3 pages2 9 4 Dissolution Test For Transdermal Patchesapi-261124906No ratings yet
- TORT PBL SubmissionDocument29 pagesTORT PBL SubmissionLam Kian Yip0% (1)
- Anatomia Del Piso de La Cámara Pulpar KRASNER JOE 2004 PDFDocument12 pagesAnatomia Del Piso de La Cámara Pulpar KRASNER JOE 2004 PDFMatthew Lama CordovaNo ratings yet
- PENGUMUMANDocument3 pagesPENGUMUMANheni arisNo ratings yet
- Diveheart Script 2022Document5 pagesDiveheart Script 2022nurliyana.roslan13493No ratings yet
- Cousins & Huffman ASM 2002Document25 pagesCousins & Huffman ASM 2002yodoidNo ratings yet
- Acs PPT Final 6-14-10Document66 pagesAcs PPT Final 6-14-10Yoseph Arif PutraNo ratings yet
- Shenimt e Mia Personale Per DDXDocument281 pagesShenimt e Mia Personale Per DDXJeronim H'gharNo ratings yet
- March 24, 2017 Strathmore TimesDocument28 pagesMarch 24, 2017 Strathmore TimesStrathmore TimesNo ratings yet
- Curriculum Vitae of DR Kiran AshokDocument4 pagesCurriculum Vitae of DR Kiran AshokkiranadrNo ratings yet
- NCP & Prio!!!Document45 pagesNCP & Prio!!!Sj 斗力上100% (1)
- Evaluación Clínica de La Eficacia Aguda de Un Preparado de Valeriana y Lúpulo en La Mejora Del SueñoDocument7 pagesEvaluación Clínica de La Eficacia Aguda de Un Preparado de Valeriana y Lúpulo en La Mejora Del SueñoGianny PastorNo ratings yet
- Indonesian Police HospitalDocument2 pagesIndonesian Police HospitalbhayangkaraNo ratings yet
- Wang Yujie ResumeDocument1 pageWang Yujie Resumeapi-314200618No ratings yet
- Raising Meat RabbitsDocument4 pagesRaising Meat RabbitsMike NichlosNo ratings yet
- Dexamethasone: Continuing EducationDocument5 pagesDexamethasone: Continuing EducationTina PatelNo ratings yet
- 6 Surgical Periodontal TherapyDocument38 pages6 Surgical Periodontal TherapyPriya SargunanNo ratings yet
- Hackenberger2012 PDFDocument7 pagesHackenberger2012 PDFWahyu FathurrachmanNo ratings yet
- Acute Respiratory Distress SyndromeDocument3 pagesAcute Respiratory Distress SyndromeJorie Roco100% (1)
- Mango LeavesDocument5 pagesMango LeavesMuthuswamy JayaramNo ratings yet
- Lee CV PDFDocument33 pagesLee CV PDFAnonymous 2g7jW7No ratings yet
- The Atlantean ConspiracyDocument35 pagesThe Atlantean Conspiracycheesehomer100% (1)
- Togas Tulandi Atlas of Laparoscopy and Hysteroscopy Techniques, Third EditionDocument189 pagesTogas Tulandi Atlas of Laparoscopy and Hysteroscopy Techniques, Third EditionSimplacean MarianaNo ratings yet
- Autoimmune Hepatitis: Robert G. Gish MDDocument53 pagesAutoimmune Hepatitis: Robert G. Gish MDRobert G. Gish, MD100% (1)