You might also like
- Neuroradiology: Kesha DesaiDocument21 pagesNeuroradiology: Kesha DesaidamaiswariNo ratings yet
- 3ST Frozen Shoulder 08Document2 pages3ST Frozen Shoulder 08damaiswariNo ratings yet
- JNeurosciRuralPract53265-4597438 124614Document4 pagesJNeurosciRuralPract53265-4597438 124614damaiswariNo ratings yet
- Referensi PDFDocument7 pagesReferensi PDFdamaiswariNo ratings yet
- Faktor Risiko Konjungtivitis Pada Bayi DGN HIVDocument14 pagesFaktor Risiko Konjungtivitis Pada Bayi DGN HIVdamaiswariNo ratings yet
- Ni Hms 194592Document15 pagesNi Hms 194592damaiswariNo ratings yet
- Pediatrics 2010 Duijts E18 25Document10 pagesPediatrics 2010 Duijts E18 25damaiswariNo ratings yet
- Epidemiology DLL Peritonsil Abses PDFDocument7 pagesEpidemiology DLL Peritonsil Abses PDFdamaiswariNo ratings yet
- Pediatrics 2014 1146 50Document7 pagesPediatrics 2014 1146 50damaiswariNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Samsung C&T AuditDocument104 pagesSamsung C&T AuditkevalNo ratings yet
- Hacking Web ApplicationsDocument5 pagesHacking Web ApplicationsDeandryn RussellNo ratings yet
- Module IV StaffingDocument3 pagesModule IV Staffingyang_19250% (1)
- Arts, Sciences& Technology University in Lebanon: Clinical Booking WebsiteDocument25 pagesArts, Sciences& Technology University in Lebanon: Clinical Booking WebsiteTony SawmaNo ratings yet
- Ap Finance Go PDFDocument3 pagesAp Finance Go PDFSuresh Babu ChinthalaNo ratings yet
- Organization Structure in SAP Plant Maintenance: CommentsDocument3 pagesOrganization Structure in SAP Plant Maintenance: CommentsMarco Antônio Claret TeixeiraNo ratings yet
- EASE Module 1 Geometric RelationsDocument26 pagesEASE Module 1 Geometric RelationsMarlon MiclatNo ratings yet
- Sec 4 RA 6713 & Sec 3 RA 3019 OutlineDocument4 pagesSec 4 RA 6713 & Sec 3 RA 3019 OutlineAivan Charles TorresNo ratings yet
- Teaching As Noble ProfessionDocument1 pageTeaching As Noble ProfessionJeric AcostaNo ratings yet
- A-7 Longitudinal SectionDocument1 pageA-7 Longitudinal SectionarjayymerleNo ratings yet
- New Monasticism: An Interspiritual Manifesto For Contemplative Life in The 21st CenturyDocument32 pagesNew Monasticism: An Interspiritual Manifesto For Contemplative Life in The 21st CenturyWorking With Oneness100% (8)
- Written Work 1 Q1 Science 10Document6 pagesWritten Work 1 Q1 Science 10JOEL MONTERDENo ratings yet
- USD - DPF Cleaning Machine - POSEYDON1000 - PolDocument8 pagesUSD - DPF Cleaning Machine - POSEYDON1000 - PolAbaidi RabieNo ratings yet
- Business ModelsDocument10 pagesBusiness ModelsPiyushNo ratings yet
- How to Stop Overthinking and Make DecisionsDocument39 pagesHow to Stop Overthinking and Make DecisionsDeepak SinghNo ratings yet
- FS1-Episode 10Document4 pagesFS1-Episode 10Mark Gerald Lagran82% (11)
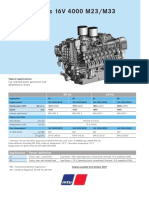
- Diesel Engines 16V 4000 M23/M33: 50 HZ 60 HZDocument2 pagesDiesel Engines 16V 4000 M23/M33: 50 HZ 60 HZAlberto100% (1)
- CartridgeDocument26 pagesCartridgeMnavya SaiNo ratings yet
- OsteoporosisDocument57 pagesOsteoporosisViviViviNo ratings yet
- Types of Companies Classified by Incorporation, Membership, Liability and ControlDocument11 pagesTypes of Companies Classified by Incorporation, Membership, Liability and ControlPrasad BulbuleNo ratings yet
- On Healing Powers: Asclepius, Caduceus and AntibodiesDocument4 pagesOn Healing Powers: Asclepius, Caduceus and AntibodiesasclepiuspdfsNo ratings yet
- Si Eft Mandate FormDocument1 pageSi Eft Mandate FormdSolarianNo ratings yet
- Petroleum Research: Khalil Shahbazi, Amir Hossein Zarei, Alireza Shahbazi, Abbas Ayatizadeh TanhaDocument15 pagesPetroleum Research: Khalil Shahbazi, Amir Hossein Zarei, Alireza Shahbazi, Abbas Ayatizadeh TanhaLibya TripoliNo ratings yet
- Diseñadores Del Siglo XX - Las Figuras Clave Del Diseño y - Dormer, Peter - 1993 - Barcelona - Ceac - 9780747202684 - Anna's ArchiveDocument264 pagesDiseñadores Del Siglo XX - Las Figuras Clave Del Diseño y - Dormer, Peter - 1993 - Barcelona - Ceac - 9780747202684 - Anna's ArchiveSilvina RodríguezNo ratings yet
- India-An Underdeveloped Economy: (Contd )Document6 pagesIndia-An Underdeveloped Economy: (Contd )Amrita Prashant IyerNo ratings yet
- Module 4 Flexible Learning EnvironmentDocument2 pagesModule 4 Flexible Learning EnvironmentRyan Contratista GimarinoNo ratings yet
- The Power of Prayer English PDFDocument312 pagesThe Power of Prayer English PDFHilario Nobre100% (1)
- Redox ChemistryDocument25 pagesRedox ChemistrySantosh G PattanadNo ratings yet
- Ky203817 PSRPT 2022-05-17 14.39.33Document8 pagesKy203817 PSRPT 2022-05-17 14.39.33Thuy AnhNo ratings yet
- Architecture Floor Plan Abbreviations AnDocument11 pagesArchitecture Floor Plan Abbreviations AnGraphitti Koncepts and DesignsNo ratings yet