You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- NP IiDocument11 pagesNP IiOlivia LowellNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Bumrungrad Hospital Case StudyDocument7 pagesBumrungrad Hospital Case StudyRaghvendra ThakurNo ratings yet
- Traditional and Alternative Medicine ActDocument13 pagesTraditional and Alternative Medicine ActAnthonette EstigoyNo ratings yet
- 201 Dowman DR, Atlanta, GA 30322Document3 pages201 Dowman DR, Atlanta, GA 30322Huy LeNo ratings yet
- Obsessive Compulsive Disorder (Matchstick Men 2003)Document8 pagesObsessive Compulsive Disorder (Matchstick Men 2003)Nauman RashidNo ratings yet
- Capstone Project Final DraftDocument11 pagesCapstone Project Final Draftapi-540888060No ratings yet
- MyChart - Test DetailsDocument2 pagesMyChart - Test DetailsLeo ShenNo ratings yet
- RadiotherapyDocument39 pagesRadiotherapykharoliyaakshitaNo ratings yet
- Ca 1-7-2100Document12 pagesCa 1-7-2100fasthospitalNo ratings yet
- Pil 880 PDFDocument6 pagesPil 880 PDFBobbyNo ratings yet
- Nursing Practice IIDocument18 pagesNursing Practice IIstuffednurseNo ratings yet
- Giving Injections: Subcutaneous (SC), Intramuscular (Im) and Intravenous (Iv) 1. PurposeDocument9 pagesGiving Injections: Subcutaneous (SC), Intramuscular (Im) and Intravenous (Iv) 1. Purposemilliondreams009No ratings yet
- Psychoanalysis and Dynamic Psychotherapy in Institutional Settings  Then and Now (Psychosis, Vol. 6, Issue 4) (2014)Document4 pagesPsychoanalysis and Dynamic Psychotherapy in Institutional Settings  Then and Now (Psychosis, Vol. 6, Issue 4) (2014)AriLauhamoNo ratings yet
- CH 0060Document7 pagesCH 0060Shreya SinhaNo ratings yet
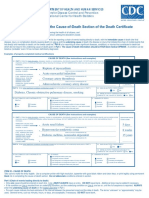
- Instructions For Completing The Cause of Death Section On Death Certificate PDFDocument2 pagesInstructions For Completing The Cause of Death Section On Death Certificate PDFpilcheritoNo ratings yet
- PRC Bonmemo No 1 B S 2009 Ip Icnb Io Performance Evaluation Forms For Cmo No 14 Graduates AnnexDocument10 pagesPRC Bonmemo No 1 B S 2009 Ip Icnb Io Performance Evaluation Forms For Cmo No 14 Graduates AnnexlylesantosNo ratings yet
- Management of Incidental Pancreatic Cysts: A White Paper of The ACR Incidental Findings CommitteeDocument13 pagesManagement of Incidental Pancreatic Cysts: A White Paper of The ACR Incidental Findings CommitteeSole GonzalezNo ratings yet
- Scrofula or King'S Evil,: Scurvy, and CancerDocument26 pagesScrofula or King'S Evil,: Scurvy, and CancerGutenberg.orgNo ratings yet
- 2-Year Savvy IMG RoadmapDocument12 pages2-Year Savvy IMG RoadmapJoshua JosephNo ratings yet
- HIV in Mothers and Children: What's New?Document5 pagesHIV in Mothers and Children: What's New?VeronikaNo ratings yet
- Lampiran 4 - IsiDocument22 pagesLampiran 4 - IsiAhmad ThotuchingNo ratings yet
- CHC Staffing Plan Procedure ExampleDocument20 pagesCHC Staffing Plan Procedure ExampleAko C Kristal100% (1)
- Antiphospholipid Syndrome in PregnancyDocument7 pagesAntiphospholipid Syndrome in PregnancyDara Dasawulansari SyamsuriNo ratings yet
- Perioperative Nursing Care 1Document17 pagesPerioperative Nursing Care 1Kristian Dave DivaNo ratings yet
- Herbal Plants (Halamang Gamot)Document25 pagesHerbal Plants (Halamang Gamot)SORENI SORENINo ratings yet
- Writing Your Personal StatementDocument6 pagesWriting Your Personal StatementBilal MohammadNo ratings yet
- Figure 1. New Criteria For AKI Diagnosis Are Displayed. in Order To Diagnose AKIDocument8 pagesFigure 1. New Criteria For AKI Diagnosis Are Displayed. in Order To Diagnose AKIMayra Alejandra Prada SerranoNo ratings yet
- Micturating Cystourethrogram (MCUG)Document8 pagesMicturating Cystourethrogram (MCUG)Hamzeh AlmasriNo ratings yet
- Traditional Chinese Medicine in Dermatology: J K & R DDocument8 pagesTraditional Chinese Medicine in Dermatology: J K & R DAndre3893No ratings yet
- 2011-02-25 FDA Approves EDARBI (Azilsartan Medoxomil) For The Treatment of HypertensionDocument3 pages2011-02-25 FDA Approves EDARBI (Azilsartan Medoxomil) For The Treatment of HypertensionShuona YuanNo ratings yet