You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Medical Auditing Training: CPMA®: Practical Application WorkbookDocument23 pagesMedical Auditing Training: CPMA®: Practical Application WorkbookAnthony El Hage0% (1)
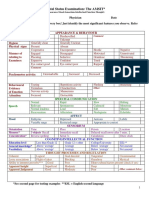
- Mental Status Examination: The AMSIT : Neat and Tidy DisshevelledDocument2 pagesMental Status Examination: The AMSIT : Neat and Tidy Disshevellednisreen100% (1)
- NP 5Document6 pagesNP 5Ana Blesilda Cachola100% (1)
- Quiz 1Document8 pagesQuiz 1murali_bharadwazNo ratings yet
- Quiz 2Document8 pagesQuiz 2murali_bharadwazNo ratings yet
- Quiz 3Document6 pagesQuiz 3murali_bharadwazNo ratings yet
- Fastigial Nuclei) .: Cerebellar LobesDocument6 pagesFastigial Nuclei) .: Cerebellar Lobesmurali_bharadwazNo ratings yet
- Medullar Oblongata (Myelencephalon) Gastrointestinal MotilityDocument10 pagesMedullar Oblongata (Myelencephalon) Gastrointestinal Motilitymurali_bharadwazNo ratings yet
- The Auditory System: NeuraxisDocument2 pagesThe Auditory System: Neuraxismurali_bharadwazNo ratings yet
- Brain Gross AnatomyDocument5 pagesBrain Gross Anatomymurali_bharadwazNo ratings yet
- Vertebral Arteries, and Their Divisions. Arteries Fuse To Form The Basilar ArteryDocument6 pagesVertebral Arteries, and Their Divisions. Arteries Fuse To Form The Basilar Arterymurali_bharadwazNo ratings yet
- Presented To CD4+ T Cells. (MCQ) Damage and The Characteristic Mucosal PathologyDocument3 pagesPresented To CD4+ T Cells. (MCQ) Damage and The Characteristic Mucosal Pathologymurali_bharadwazNo ratings yet
- 33 Polycystic Kidney DiseaseDocument2 pages33 Polycystic Kidney Diseasemurali_bharadwaz100% (1)
- Aiims May 2013 Transfer 6Document6 pagesAiims May 2013 Transfer 6murali_bharadwazNo ratings yet
- Aiims May 2013 Transfer 6Document6 pagesAiims May 2013 Transfer 6murali_bharadwazNo ratings yet
- 1 Contraception Part 1Document9 pages1 Contraception Part 1murali_bharadwazNo ratings yet
- Red Cells or White Cells.: g/100 Ml. (MCQ)Document7 pagesRed Cells or White Cells.: g/100 Ml. (MCQ)murali_bharadwazNo ratings yet
- 33 Polycystic Kidney DiseaseDocument2 pages33 Polycystic Kidney Diseasemurali_bharadwaz100% (1)
- RickricketsDocument30 pagesRickricketsmurali_bharadwazNo ratings yet
- Celiac Disease PresentationDocument24 pagesCeliac Disease Presentationmurali_bharadwazNo ratings yet
- DR Murali Bharadwaz Classes For APPGDocument6 pagesDR Murali Bharadwaz Classes For APPGmurali_bharadwazNo ratings yet
- Evaluation of Psychiatric Disorders: Key ConceptsDocument12 pagesEvaluation of Psychiatric Disorders: Key ConceptsraniNo ratings yet
- Clinical Interviewing SkillsDocument27 pagesClinical Interviewing SkillsAcademic Committe100% (1)
- MHN MUHS External and InternalDocument5 pagesMHN MUHS External and Internalanupa sukalikarNo ratings yet
- VCNS122 Studyguide 2021Document19 pagesVCNS122 Studyguide 2021yarec79954No ratings yet
- Fundamentals of Abnormal Psychology 8th Edition Comer Test Bank 1Document32 pagesFundamentals of Abnormal Psychology 8th Edition Comer Test Bank 1michael100% (41)
- Initial Mental Status ExamDocument6 pagesInitial Mental Status ExamYanna N. CuakiNo ratings yet
- 13 Areas of Assessment BGHDocument2 pages13 Areas of Assessment BGHZamranosNo ratings yet
- Schizophrenia: Signs and SymptomsDocument38 pagesSchizophrenia: Signs and SymptomsRatu Nurul Fadhilah100% (1)
- Neuro AssessmentDocument39 pagesNeuro AssessmentkixfrondaNo ratings yet
- Case Taking TIPPS4Document42 pagesCase Taking TIPPS4Anamika Sinha100% (1)
- Mental Health Status Exam Cheat Sheet ICANotesDocument7 pagesMental Health Status Exam Cheat Sheet ICANotesSanober Memon100% (1)
- Subjective Data: "Mag Lisud Raba Na Siya Og Storya Unya Magka Rumble Ang Mga Words " As Verbalized by The CaregiverDocument6 pagesSubjective Data: "Mag Lisud Raba Na Siya Og Storya Unya Magka Rumble Ang Mga Words " As Verbalized by The CaregiverflorenzoNo ratings yet
- Risk Assessment in PsychiatryDocument56 pagesRisk Assessment in PsychiatryAmin ZahariNo ratings yet
- Sensation, Perception, and CognitionDocument55 pagesSensation, Perception, and CognitionRikha ParamittaNo ratings yet
- Psychiatry Notes and Other Stations Including NNDocument82 pagesPsychiatry Notes and Other Stations Including NNAdnan Al JafaryNo ratings yet
- Nimra CasesDocument34 pagesNimra Casesua9985872No ratings yet
- Bipolar Disorder in Postpartum Women - Epidemiology, Clinical Features, Assessment, and Diagnosis PDFDocument14 pagesBipolar Disorder in Postpartum Women - Epidemiology, Clinical Features, Assessment, and Diagnosis PDFdreamingNo ratings yet
- Mental Status ExamDocument7 pagesMental Status ExamDanielle BanNo ratings yet
- Mental Status ExaminationDocument7 pagesMental Status ExaminationUdaya Sree100% (4)
- Chapter 4 Assessment of Abnormal BehaviourDocument61 pagesChapter 4 Assessment of Abnormal BehaviourEsraRamosNo ratings yet
- Ebook Neurology For The Non Neurologist Volume 103 Issue 2 April 3 2019 - 0323654711 - Elsevier PDF Full Chapter PDFDocument78 pagesEbook Neurology For The Non Neurologist Volume 103 Issue 2 April 3 2019 - 0323654711 - Elsevier PDF Full Chapter PDFbonnie.xiong249100% (32)
- Mental Status ExaminationDocument5 pagesMental Status Examinationfreya_28100% (1)
- Jurnal Jiwa 4Document10 pagesJurnal Jiwa 4Bella FebriantiNo ratings yet
- Outline of Mental Status ExaminationDocument10 pagesOutline of Mental Status ExaminationMohammed Hosen100% (1)
- 14 - Neuropsychological AssessmentDocument14 pages14 - Neuropsychological AssessmentMARIE ROSE L. FUNTANARNo ratings yet
- Psychiatric Interview & Mental Status ExamDocument36 pagesPsychiatric Interview & Mental Status Examsarguss1494% (16)
- Assessing Appearance and Mental StatusDocument12 pagesAssessing Appearance and Mental StatusAaron Perez SubidaNo ratings yet