You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Urinary Tract Infection & PyelonephritisDocument3 pagesUrinary Tract Infection & PyelonephritisUsman Ali AkbarNo ratings yet
- Chronic Renal Failure: Concise Long Case ApproachDocument3 pagesChronic Renal Failure: Concise Long Case ApproachUsman Ali AkbarNo ratings yet
- Renal Tubular Acidosis Summary - AdjDocument1 pageRenal Tubular Acidosis Summary - AdjUsman Ali AkbarNo ratings yet
- Polycystic Kidneys: Adult PKD: ComplicationsDocument1 pagePolycystic Kidneys: Adult PKD: ComplicationsUsman Ali AkbarNo ratings yet
- GI Bleeding Team Work - 2nd EditionDocument9 pagesGI Bleeding Team Work - 2nd EditionUsman Ali AkbarNo ratings yet
- Obstructive Airway Disease: Dr. Khalid Al-Mobaireek King Khalid University HospitalDocument53 pagesObstructive Airway Disease: Dr. Khalid Al-Mobaireek King Khalid University HospitalUsman Ali AkbarNo ratings yet
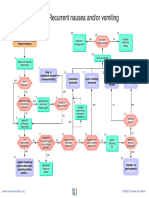
- Recurrent Nausea Andor VomitingDocument8 pagesRecurrent Nausea Andor VomitingUsman Ali AkbarNo ratings yet
- DialysisDocument2 pagesDialysisUsman Ali AkbarNo ratings yet
- King Khalid University Hospital Department of Obstetrics & Gyncology Course 481Document40 pagesKing Khalid University Hospital Department of Obstetrics & Gyncology Course 481Usman Ali AkbarNo ratings yet
- Recurrent VomitingDocument16 pagesRecurrent VomitingUsman Ali AkbarNo ratings yet
- Anaemia in PregnancyDocument13 pagesAnaemia in PregnancyUsman Ali AkbarNo ratings yet
- DR Othman Alharbi, MBBS FRCPC Assistance Professor & Consultant Gastroenterology College of Medicine King Saud UniversityDocument18 pagesDR Othman Alharbi, MBBS FRCPC Assistance Professor & Consultant Gastroenterology College of Medicine King Saud UniversityUsman Ali AkbarNo ratings yet
- Organophosphate PoisoningDocument23 pagesOrganophosphate PoisoningUsman Ali AkbarNo ratings yet
- Through The Strange WindsDocument5 pagesThrough The Strange WindsUsman Ali AkbarNo ratings yet
- Cord ProlapseDocument2 pagesCord ProlapseUsman Ali AkbarNo ratings yet
- When Hope DiesDocument2 pagesWhen Hope DiesUsman Ali AkbarNo ratings yet
- Subject: Permission For Badminton Court NID, Multan: TH THDocument1 pageSubject: Permission For Badminton Court NID, Multan: TH THUsman Ali AkbarNo ratings yet
- GRAM NEGATIVE RODS (5) Fastidious Organisms From Animal Sources (A)Document1 pageGRAM NEGATIVE RODS (5) Fastidious Organisms From Animal Sources (A)Usman Ali AkbarNo ratings yet
- Alas!! EmpytinessDocument2 pagesAlas!! EmpytinessUsman Ali AkbarNo ratings yet
- Untold Stanza... : - Nasim Alam (N-61)Document1 pageUntold Stanza... : - Nasim Alam (N-61)Usman Ali AkbarNo ratings yet
- Lect 1:: M2Pasysl21 Urinary SystemDocument4 pagesLect 1:: M2Pasysl21 Urinary SystemUsman Ali AkbarNo ratings yet
- Death and The Mother For MergeDocument4 pagesDeath and The Mother For MergeUsman Ali AkbarNo ratings yet
- AHIST (WA Unit 1)Document4 pagesAHIST (WA Unit 1)Min Kaung San133No ratings yet
- Spark Timer LabDocument4 pagesSpark Timer LabKshitiz Vijayvargiya100% (1)
- Minor Project On Technical Analysis of Banking SectorDocument28 pagesMinor Project On Technical Analysis of Banking SectorShadman TauheedNo ratings yet
- Draft Motion Quash - Sandiganbayan-2 InformationDocument10 pagesDraft Motion Quash - Sandiganbayan-2 Informationkei baligodNo ratings yet
- Content EvaluationDocument3 pagesContent EvaluationRIPUDAMAN SINGHNo ratings yet
- PradaDocument4 pagesPradaMJ Villamor AquilloNo ratings yet
- Maternal and Child HealthDocument62 pagesMaternal and Child HealthAsfand KhanNo ratings yet
- Guidelines For Setting Up Custody Transfer Metering Station at Entry and Exit Points PDFDocument90 pagesGuidelines For Setting Up Custody Transfer Metering Station at Entry and Exit Points PDFjemorenoa8954No ratings yet
- Romeo and Juliet: GradeDocument128 pagesRomeo and Juliet: GradeJunior MohaleNo ratings yet
- Title: GPS: Global Positioning SystemDocument18 pagesTitle: GPS: Global Positioning SystemBa HoNo ratings yet
- 625 Characterization of Microstructures in Inconel 625 Using X-RAY PDFDocument5 pages625 Characterization of Microstructures in Inconel 625 Using X-RAY PDFKara WhiteNo ratings yet
- Apology: By: PlatoDocument3 pagesApology: By: PlatoGermaine Aliangan100% (1)
- DLL - Aug 28-Sept 1Document6 pagesDLL - Aug 28-Sept 1Benes Salamanca BolascoNo ratings yet
- Course Syllabus ECE 635 - Error Detecting and Correcting Systems DesignDocument3 pagesCourse Syllabus ECE 635 - Error Detecting and Correcting Systems DesignPrashant PatavardhanNo ratings yet
- The Type-Variety Smith, Willey y GiffordDocument12 pagesThe Type-Variety Smith, Willey y GiffordMiguel Roberto Guevara ChumaceroNo ratings yet
- Mirzoeff, Nicholas. The Right To LookDocument25 pagesMirzoeff, Nicholas. The Right To LookPaula Cardoso PereiraNo ratings yet
- DjvuDocument49 pagesDjvugaud28No ratings yet
- Piramal Glass - Rights Issue - Aug 2009Document311 pagesPiramal Glass - Rights Issue - Aug 2009vishmittNo ratings yet
- The Robber BridegroomDocument4 pagesThe Robber BridegroomKuberNo ratings yet
- Mother Country Catherine HallDocument7 pagesMother Country Catherine HallStephen BeckerNo ratings yet
- Q2 MODULE3 G11 .NET PROG MangaldanNHSDocument10 pagesQ2 MODULE3 G11 .NET PROG MangaldanNHSJensen TagudinNo ratings yet
- Transfer Learning PDFDocument10 pagesTransfer Learning PDFajaytiwari2779No ratings yet
- Sample Qualitative PHD ThesisDocument5 pagesSample Qualitative PHD ThesisFindSomeoneToWriteMyPaperSingapore100% (2)
- Straight Lines - WorkbookDocument37 pagesStraight Lines - WorkbookKarthikeyanNo ratings yet
- VivitrolFactSheet PDFDocument5 pagesVivitrolFactSheet PDFwebmaster@drugpolicy.org100% (1)
- Eng. McqsDocument3 pagesEng. McqsJawad Ur Rehman BhuttaNo ratings yet
- Exp. 1.8 (Form 5)Document2 pagesExp. 1.8 (Form 5)IMELDANo ratings yet
- 1 s2.0 S187705092102425X MainDocument9 pages1 s2.0 S187705092102425X MainMichael Angelo AlbaoNo ratings yet
- Essays (No More Than 500 Words) Paragraphs, Single SpacedDocument2 pagesEssays (No More Than 500 Words) Paragraphs, Single SpacedDuy Lê HữuNo ratings yet
- Engine, Lubrication: CautionDocument26 pagesEngine, Lubrication: CautionBenNo ratings yet