You might also like
- Fdar Samples PresentationDocument29 pagesFdar Samples PresentationKewkew Azilear89% (38)
- FDAR (Sample)Document3 pagesFDAR (Sample)Zarah Joy Tabuyan88% (17)
- Fdar Samples PresentationDocument29 pagesFdar Samples PresentationAnnette Aquino Guevarra100% (2)
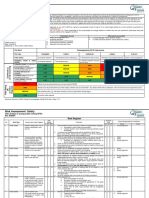
- 015-Lifting Plan Method & Risk AssessmentDocument3 pages015-Lifting Plan Method & Risk AssessmentMAB AliNo ratings yet
- FDARDocument33 pagesFDARRaquel M. Mendoza100% (7)
- Fdar 3Document17 pagesFdar 3leslie_macasaet75% (4)
- Date/Time Focus Progress Notes: Charisse Dl. LimosDocument6 pagesDate/Time Focus Progress Notes: Charisse Dl. LimosCharisse Limos100% (6)
- Fdar Charting (Umali)Document6 pagesFdar Charting (Umali)NicholeGarcesCisnerosNo ratings yet
- D-Patient Verbalized "Sakit Gyod Akong Tiyan", Pain: Sample 1Document29 pagesD-Patient Verbalized "Sakit Gyod Akong Tiyan", Pain: Sample 1jaypee100% (3)
- FDARDocument5 pagesFDARKris TejereroNo ratings yet
- Sample Dar ChartingDocument3 pagesSample Dar ChartingAl Lakah75% (4)
- Fdar CompilationsDocument3 pagesFdar Compilationsjp_ibañez67% (3)
- Risk Assessmet Young PeopleDocument3 pagesRisk Assessmet Young PeopleParmod RanaNo ratings yet
- Focus ChartingDocument46 pagesFocus ChartingIsmail Alnemr100% (5)
- D Received Patient Sitting On Bed With Bottle #Document17 pagesD Received Patient Sitting On Bed With Bottle #jaypee100% (2)
- Focus Charting of FDocument12 pagesFocus Charting of FRobert Rivas0% (2)
- Fdar Charting - WadinganDocument1 pageFdar Charting - WadinganSkai JeonNo ratings yet
- Character, Onset, Location, Duration, Severity, Pattern and Associated - FactorsDocument1 pageCharacter, Onset, Location, Duration, Severity, Pattern and Associated - FactorsJohn CuencoNo ratings yet
- Sample Nurses Notes CuDocument3 pagesSample Nurses Notes Cuapi-1978086589% (19)
- Nurses NotesDocument1 pageNurses Notesmona_javier100% (4)
- Cast CareDocument1 pageCast CareCarmelita SaltNo ratings yet
- Pastry War Agave Captains ListDocument6 pagesPastry War Agave Captains ListdavidjmontgomeryNo ratings yet
- FDAR ChartingDocument2 pagesFDAR ChartingRaisah Bint Abdullah100% (1)
- Dona Remedios Trinidad Romualdez Medical Foundation College of NursingDocument3 pagesDona Remedios Trinidad Romualdez Medical Foundation College of NursingRoyce Vincent Tizon100% (3)
- Focus ChartingDocument15 pagesFocus ChartingBobby Potestas Escalante83% (6)
- Focus ChartingDocument2 pagesFocus ChartingJane Umali Tulabot83% (6)
- Hyperthermia: Date/Hour Focus Progress NotesDocument11 pagesHyperthermia: Date/Hour Focus Progress NotesCai Sumayod Delloro100% (3)
- Lester Fdar MarchDocument4 pagesLester Fdar MarchLeanne Joie LozanoNo ratings yet
- FdarDocument33 pagesFdarTatiana's Couture100% (2)
- FdarDocument4 pagesFdarCecile DavantesNo ratings yet
- Fdarcharting 120314214902 Phpapp02Document5 pagesFdarcharting 120314214902 Phpapp02John Louie SolitarioNo ratings yet
- SOAPIE and FDAR ChartingDocument14 pagesSOAPIE and FDAR ChartingMikaela Gabrielle GERALINo ratings yet
- Nurse'S Notes: Bautista A 58 2021-0000025 Milagros F Medical Ward-207Document5 pagesNurse'S Notes: Bautista A 58 2021-0000025 Milagros F Medical Ward-207Renea Joy ArruejoNo ratings yet
- FDAR ChartingDocument50 pagesFDAR ChartingNathaniel PulidoNo ratings yet
- Focus Charting (DAR)Document1 pageFocus Charting (DAR)Raisa Robelle QuichoNo ratings yet
- D Received Patient Sitting On Bed With Bottle # 1DDocument24 pagesD Received Patient Sitting On Bed With Bottle # 1DMai Love100% (5)
- Narrative ChartingDocument2 pagesNarrative Chartingearl_llamas0% (2)
- 12/07/20 3PM-11PM: Fdar ChartingDocument5 pages12/07/20 3PM-11PM: Fdar ChartingElle ctricaNo ratings yet
- Nurses' Notes and Treatment Record: Date/Time Focus Progress Notes (D-Data A-Action R-Response)Document2 pagesNurses' Notes and Treatment Record: Date/Time Focus Progress Notes (D-Data A-Action R-Response)Jamie Lee100% (2)
- SAMPLE FDAR CHARTING PainDocument1 pageSAMPLE FDAR CHARTING Painjpm100% (1)
- Focus ChartingDocument2 pagesFocus ChartingIrvin John Diao Capistrano100% (1)
- FDARDocument2 pagesFDARRafael Basa100% (1)
- Mendoza, Joshua G.Document7 pagesMendoza, Joshua G.Joshua MendozaNo ratings yet
- Fdar Charting and Discharge PlanningDocument2 pagesFdar Charting and Discharge PlanningFaine Angela Caones100% (1)
- FDAR Charting Sample: Date and Time Focus Data, Action, Response 12/30/14 8:00pm Post-OperativeDocument3 pagesFDAR Charting Sample: Date and Time Focus Data, Action, Response 12/30/14 8:00pm Post-OperativeNeojoy Zero-twoNo ratings yet
- Fdar Charting: Date, Time, and Shift Focus Progress NotesDocument1 pageFdar Charting: Date, Time, and Shift Focus Progress NotesBlessyl Mae EstenzoNo ratings yet
- Grand Case Pres FDARDocument11 pagesGrand Case Pres FDARMika SaldañaNo ratings yet
- Annalyn B. Forio, RN, MAN: Fdar-DocumentationDocument25 pagesAnnalyn B. Forio, RN, MAN: Fdar-Documentationjay kusainNo ratings yet
- DAR ChartingDocument2 pagesDAR ChartingJed Visaya83% (6)
- Focus Charting of FDocument12 pagesFocus Charting of FLester GonzalesNo ratings yet
- Fdar - 2 HypertensionDocument12 pagesFdar - 2 HypertensionGinena Belarmino100% (3)
- Lec - Mid WK 2Document3 pagesLec - Mid WK 2cheryl.c.miguelNo ratings yet
- FDARDocument5 pagesFDARbash021No ratings yet
- MS Simulation NotesDocument23 pagesMS Simulation NotesRegina Vyn J. MARTINEZNo ratings yet
- FNP Lec TransesDocument12 pagesFNP Lec Transesleilavesagas222No ratings yet
- FINAL OSSAM-ICU PrestudyDocument36 pagesFINAL OSSAM-ICU PrestudyHannah DuyagNo ratings yet
- F Dar KK ConDocument44 pagesF Dar KK ConhrithiksankarNo ratings yet
- Documentation System Focus ChartingDocument26 pagesDocumentation System Focus ChartingneehoshiNo ratings yet
- Focus Charting 2Document65 pagesFocus Charting 2Ella Caro100% (1)
- FDAR ChartingDocument2 pagesFDAR Chartinglouie roderosNo ratings yet
- Focus Charting Review PDFDocument9 pagesFocus Charting Review PDFTenIs ForMeNo ratings yet
- FUNDADocument6 pagesFUNDAkhayceemeade2No ratings yet
- FDARDocument22 pagesFDARzhaimeangirlNo ratings yet
- FDARDocument41 pagesFDARJojo Justo100% (2)
- Lyrics Cry2 D Boys Goodbye BabyDocument5 pagesLyrics Cry2 D Boys Goodbye BabyCarmelita SaltNo ratings yet
- Psychia Ncp-MetchelDocument9 pagesPsychia Ncp-MetchelCarmelita SaltNo ratings yet
- Theory, Building Blocks, Types, Conceptual Framework, Conceptual & Schematic ModelDocument2 pagesTheory, Building Blocks, Types, Conceptual Framework, Conceptual & Schematic ModelCarmelita Salt83% (6)
- Aseptic TechniqueDocument3 pagesAseptic TechniquedubhieNo ratings yet
- Perioperative NursingDocument18 pagesPerioperative Nursinglagunda100% (2)
- Or AttireDocument5 pagesOr AttireCarmelita SaltNo ratings yet
- Surgical InstrumentsDocument7 pagesSurgical InstrumentsCarmelita SaltNo ratings yet
- KardexDocument2 pagesKardexCarmelita SaltNo ratings yet
- Farm PowerDocument16 pagesFarm PowerJOPAKNo ratings yet
- Download Pathophysiology The Biologic Basis For Disease In Adults And Children Kathryn L Mccance Sue E Huether 2019 8Th Ed 8Th Edition Pathophysiology The Biologic Basis For Disease In Adults And Children full chapter pdf scribdDocument68 pagesDownload Pathophysiology The Biologic Basis For Disease In Adults And Children Kathryn L Mccance Sue E Huether 2019 8Th Ed 8Th Edition Pathophysiology The Biologic Basis For Disease In Adults And Children full chapter pdf scribdjames.bishop563100% (4)
- Wran WraqDocument2 pagesWran WraqJanoNo ratings yet
- Traditional and Modern Self OutlookDocument3 pagesTraditional and Modern Self Outlookethan philasia90% (10)
- Arun Ice Cream Strategic Management Case StudyDocument18 pagesArun Ice Cream Strategic Management Case Studyvar18111989100% (1)
- №2 Инструкция по эксплуатации двигателя Mitsubishi L2A, L2C, L2B, L3A, L3C, L3E (Operation manual)Document42 pages№2 Инструкция по эксплуатации двигателя Mitsubishi L2A, L2C, L2B, L3A, L3C, L3E (Operation manual)Николай НекрасовNo ratings yet
- Method Sublevel CavingDocument16 pagesMethod Sublevel CavingAntonioJavierOstosMachadoNo ratings yet
- Kit Fxloop150 Revc enDocument12 pagesKit Fxloop150 Revc enRodrigoNo ratings yet
- Manual Vibration Switch 440450 Doc 90018 031 NDocument16 pagesManual Vibration Switch 440450 Doc 90018 031 NAmiruddin Abdul RahimNo ratings yet
- Test 3 With SolutionsDocument33 pagesTest 3 With SolutionssvsvsvsvNo ratings yet
- The Fall of The House of UsherDocument9 pagesThe Fall of The House of UsherHelena GradiskiNo ratings yet
- SCOPE of Plant AuditDocument2 pagesSCOPE of Plant AuditaroontpeNo ratings yet
- Honda XR250 R XR 250 Owners Maintenance ManualDocument88 pagesHonda XR250 R XR 250 Owners Maintenance Manualcrawdoogie100% (2)
- Eco FriendlyDocument50 pagesEco FriendlySivakumar K100% (1)
- Form5 PTDocument2 pagesForm5 PTShilpa KapoorNo ratings yet
- Zolsoma 5 MG: Doctor Notes/DiagnosisDocument2 pagesZolsoma 5 MG: Doctor Notes/DiagnosisVickyNo ratings yet
- Garg Brothers & Co. Case: Managing Foreign Exchange Risk Using DerivativesDocument12 pagesGarg Brothers & Co. Case: Managing Foreign Exchange Risk Using DerivativesKanishq BawejaNo ratings yet
- HRM Bpoland.Document9 pagesHRM Bpoland.SIDDHARTH PALNo ratings yet
- Are U Trying To Switch JobDocument5 pagesAre U Trying To Switch JobJesseNo ratings yet
- Kendriya Vidyalaya Sambalpur: Science Project SESSION 2016-17 Topic-Fishes Pujarani Behera Ix - C 16 S.S.Bhoi SirDocument8 pagesKendriya Vidyalaya Sambalpur: Science Project SESSION 2016-17 Topic-Fishes Pujarani Behera Ix - C 16 S.S.Bhoi SirNiranjan BeheraNo ratings yet
- Acetyl C NeuronDocument14 pagesAcetyl C NeuronidjacobsNo ratings yet
- FAW ScriptDocument6 pagesFAW ScriptKVK East Khasi hillsNo ratings yet
- St. Anthony's College Nursing Department San Jose, AntiqueDocument30 pagesSt. Anthony's College Nursing Department San Jose, AntiqueTweenie DalumpinesNo ratings yet
- Pastor Gonzalo G. Pe Jr. Pastor Gonzalo G. Pe JR.: Date DateDocument1 pagePastor Gonzalo G. Pe Jr. Pastor Gonzalo G. Pe JR.: Date DateJewel Alayon CondinoNo ratings yet
- Plastic Technology Anna Univ 6 SemestwrDocument13 pagesPlastic Technology Anna Univ 6 SemestwrAabraham Samraj PonmaniNo ratings yet
- CH110 Tutorial SHEET 8 - Organic ChemistryDocument10 pagesCH110 Tutorial SHEET 8 - Organic ChemistryJames MukopaNo ratings yet
- Toledo Power Company: Terms of ReferenceDocument8 pagesToledo Power Company: Terms of Referencejet toledo100% (1)