You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- IssaDocument31 pagesIssaNayeem100% (1)
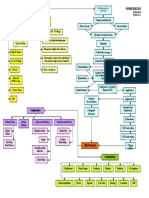
- Hypertension Concept MapDocument1 pageHypertension Concept Mapashleydean100% (7)
- BSN 3F 2B Ectopic Pregnancy PIH Case PresDocument47 pagesBSN 3F 2B Ectopic Pregnancy PIH Case PresKenji ToleroNo ratings yet
- Calculation NCM 105 FinalsDocument6 pagesCalculation NCM 105 FinalsMa. Christina ConcepcionNo ratings yet
- Nursing Care Process Case StudyDocument6 pagesNursing Care Process Case StudyEunice RosalesNo ratings yet
- Coversam 4mg/5mg Tablets Coversam 4mg/10mg Tablets Coversam 8mg/5mg Tablets Coversam 8mg/10mg TabletsDocument2 pagesCoversam 4mg/5mg Tablets Coversam 4mg/10mg Tablets Coversam 8mg/5mg Tablets Coversam 8mg/10mg TabletsRaheel Neo AhmadNo ratings yet
- Overview of Hypertension in Adults - Uptodate FreeDocument32 pagesOverview of Hypertension in Adults - Uptodate FreedrsadafrafiNo ratings yet
- High Blood PressureDocument9 pagesHigh Blood PressureshashidharanNo ratings yet
- APSGNDocument3 pagesAPSGNmadimadi11No ratings yet
- CARDIODocument34 pagesCARDIOKevin Patrick PadolinaNo ratings yet
- Special Issues in The Delivery of Transcultural Nursing CareDocument32 pagesSpecial Issues in The Delivery of Transcultural Nursing CareMushtaq Ali100% (13)
- Hypertension: "The Silent Killer" Because It Generally Has No Symptoms Until Serious Complications DevelopDocument24 pagesHypertension: "The Silent Killer" Because It Generally Has No Symptoms Until Serious Complications Developmaryam ijazNo ratings yet
- Hypertension in Dialysis PatientsDocument16 pagesHypertension in Dialysis PatientsLiliana WoodNo ratings yet
- Dover 3000 ReviewerDocument30 pagesDover 3000 ReviewerroseNo ratings yet
- 10.1007@s11325 012 0746 7Document8 pages10.1007@s11325 012 0746 7GissellePantojaNo ratings yet
- Drug Treatment of Hypertension in PregnancyDocument15 pagesDrug Treatment of Hypertension in PregnancytetriNo ratings yet
- Hypertension and Head Injury: Current Hypertension Reports January 2006Document5 pagesHypertension and Head Injury: Current Hypertension Reports January 2006Yen NgoNo ratings yet
- Prentice9e Im Chap23Document8 pagesPrentice9e Im Chap23api-281340024100% (1)
- Palembang Cardiology Update X Registration 2019 05-20-07!59!36 674Document5 pagesPalembang Cardiology Update X Registration 2019 05-20-07!59!36 674Fachrezi KhatamiNo ratings yet
- Young and Middle Adulthood Nutrition ReportDocument50 pagesYoung and Middle Adulthood Nutrition ReportFabby Vitacion TanNo ratings yet
- Lab Report - Circulation and RespirationDocument4 pagesLab Report - Circulation and RespirationSimranNo ratings yet
- Amazing Health Benefits of Bone Broth!Document21 pagesAmazing Health Benefits of Bone Broth!NirvanajunctureNo ratings yet
- Flip Chart - My Health Is My Responsibility EnglishDocument28 pagesFlip Chart - My Health Is My Responsibility EnglishlivelinamiNo ratings yet
- Family Nursing Care PlanDocument2 pagesFamily Nursing Care Plankaycelyn jimenezNo ratings yet
- Clinmed 21 3 E275Document8 pagesClinmed 21 3 E275Carlos CoronaNo ratings yet
- Cardiology Curriculum LatestDocument31 pagesCardiology Curriculum LatestKrishNo ratings yet
- GSK Sotrovimab Fact Sheet For HCP 12222021Document34 pagesGSK Sotrovimab Fact Sheet For HCP 12222021Jillian SmithNo ratings yet
- Volpe 2013 - Magnesium in Disease Prevention and Overall HealthDocument6 pagesVolpe 2013 - Magnesium in Disease Prevention and Overall HealthAlbert CalvetNo ratings yet
- AntihypertensiveDocument163 pagesAntihypertensiveOsama FrancisNo ratings yet
- Dialogue On Medical Surgical NursingDocument3 pagesDialogue On Medical Surgical NursingAnonymous XEV3a17n3YNo ratings yet