You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Case Taking ProformaDocument7 pagesCase Taking ProformaDr Dushyant Kamal Dhari50% (2)
- HSE Management System ManualDocument6 pagesHSE Management System Manualasma100% (1)
- 201210221219130.laporan Eia Damansara-Shah Alam Elevated Highway-Ukmpakarunding PDFDocument480 pages201210221219130.laporan Eia Damansara-Shah Alam Elevated Highway-Ukmpakarunding PDFmanimaran75100% (1)
- Diagnosis AutismDocument6 pagesDiagnosis AutismDr Dushyant Kamal DhariNo ratings yet
- List of InstitutesDocument30 pagesList of InstitutesDr Dushyant Kamal DhariNo ratings yet
- Syzygium CuminiDocument13 pagesSyzygium CuminiDr Dushyant Kamal DhariNo ratings yet
- An Interview With Henny HeudensDocument7 pagesAn Interview With Henny HeudensDr Dushyant Kamal Dhari100% (1)
- Rheumatic Eye - A RepertoryDocument5 pagesRheumatic Eye - A RepertoryDr Dushyant Kamal DhariNo ratings yet
- AnxietyDocument176 pagesAnxietyDr Dushyant Kamal Dhari100% (3)
- WHO Dengue Guidelines 2013Document160 pagesWHO Dengue Guidelines 2013Jason MirasolNo ratings yet
- Homoeopathic Management of Anxiety Disorders With The Help oDocument240 pagesHomoeopathic Management of Anxiety Disorders With The Help oDr Dushyant Kamal Dhari100% (1)
- Indian Medicinal Plants in DiabetesDocument6 pagesIndian Medicinal Plants in DiabetesDr Dushyant Kamal DhariNo ratings yet
- Rheumatic EyeDocument10 pagesRheumatic EyeDr Dushyant Kamal DhariNo ratings yet
- 5 Most Restless Remedies of MMDocument1 page5 Most Restless Remedies of MMDr Dushyant Kamal DhariNo ratings yet
- Aloe Vera MiracleDocument20 pagesAloe Vera Miracleanon-287110100% (19)
- The LM Potencies in Homeopathy: From The Beginnings To The Present DayDocument89 pagesThe LM Potencies in Homeopathy: From The Beginnings To The Present DayPrabhat Tandon100% (5)
- Vinca Rose As Anti DiabeticDocument6 pagesVinca Rose As Anti DiabeticDr Dushyant Kamal DhariNo ratings yet
- LM Potency in Fibromyalgia 2004Document6 pagesLM Potency in Fibromyalgia 2004Dr. Nancy MalikNo ratings yet
- Fenugreek On DiabetesDocument3 pagesFenugreek On DiabetesDr Dushyant Kamal DhariNo ratings yet
- Training Plan VCI TemplateDocument67 pagesTraining Plan VCI TemplateJohn Cesar Cam AntiqueNo ratings yet
- Longevity Paradox - Steven GundryDocument10 pagesLongevity Paradox - Steven Gundrysimas75% (4)
- Errors and The CBC Result 2.0Document43 pagesErrors and The CBC Result 2.0Ella OrtegaNo ratings yet
- Aster Cmi - BrochureDocument4 pagesAster Cmi - BrochureholysaatanNo ratings yet
- Assessing The Validity and Reliability of Diagnostic and Screening TestsDocument38 pagesAssessing The Validity and Reliability of Diagnostic and Screening Testssarguss1467% (3)
- Jonathan Sudharta e - PrescriptionDocument53 pagesJonathan Sudharta e - PrescriptionAchmad FachryNo ratings yet
- Duke SOM 2016-2017Document266 pagesDuke SOM 2016-2017chocolatec00kieNo ratings yet
- Frank Straub ResumeDocument6 pagesFrank Straub ResumeInlanderChrisNo ratings yet
- Life Care Medi'Call ServiceDocument5 pagesLife Care Medi'Call ServiceRajeev MehraNo ratings yet
- Norme SangeDocument2 pagesNorme SangePS NINo ratings yet
- Cowpea Isoflavones and PCOSDocument6 pagesCowpea Isoflavones and PCOSAamer SyedNo ratings yet
- Interviewing and Counseling 2023 Set - 075741Document5 pagesInterviewing and Counseling 2023 Set - 075741henri kaneNo ratings yet
- Etyl Mercaptan MSDSDocument24 pagesEtyl Mercaptan MSDSmostafa_1000100% (1)
- OCD and Psychological ManagementDocument35 pagesOCD and Psychological Managementhelal100% (1)
- SOP For Biological Safety Cabinet OperationDocument3 pagesSOP For Biological Safety Cabinet OperationMulayam Singh YadavNo ratings yet
- Toolbox Talk 07 Slips Trips FallsDocument1 pageToolbox Talk 07 Slips Trips FallsSohailNo ratings yet
- Enact Law For Ram Temple: Togadia: TimesDocument1 pageEnact Law For Ram Temple: Togadia: TimesDhanush KumarNo ratings yet
- Neonatal PneumoniaDocument2 pagesNeonatal PneumoniaJustin EduardoNo ratings yet
- Healthcare Project in AdidomeDocument20 pagesHealthcare Project in Adidomeamode idowuNo ratings yet
- Cushing'S Syndrome and Cushing'S Disease: Your Questions AnsweredDocument9 pagesCushing'S Syndrome and Cushing'S Disease: Your Questions Answeredmawarni siahaanNo ratings yet
- Domestic Workers ActDocument5 pagesDomestic Workers ActTroy San MarNo ratings yet
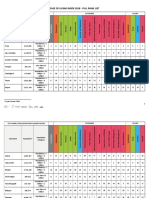
- Ease of Living Index 2018 Full Rank List PDFDocument13 pagesEase of Living Index 2018 Full Rank List PDFpraveench1888No ratings yet
- Basic Ethical Concepts To Ethical Principles: C. Personalized SexualityDocument14 pagesBasic Ethical Concepts To Ethical Principles: C. Personalized SexualitySophia BonifacioNo ratings yet
- AbiomedDocument2 pagesAbiomedVivien ZhengNo ratings yet
- Geraldine Gabriel: Work ExperienceDocument2 pagesGeraldine Gabriel: Work ExperienceSiddharth NelsonNo ratings yet
- Odontogenic Tumor PDFDocument93 pagesOdontogenic Tumor PDFEmad Alriashy100% (1)
- Allogeneic Stem Cell Transplantation - M. Laughlin, H. Lazarus (Humana, 2003) WWDocument466 pagesAllogeneic Stem Cell Transplantation - M. Laughlin, H. Lazarus (Humana, 2003) WWSerah LightNo ratings yet
- ImmunityDocument47 pagesImmunitySabCoolNo ratings yet