You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- SPADocument1 pageSPAxdmhundz999No ratings yet
- Chaotic Sword GodDocument1,928 pagesChaotic Sword Godxdmhundz999100% (1)
- 2return of The Former Hero (Fin)Document306 pages2return of The Former Hero (Fin)xdmhundz999No ratings yet
- World of CultivationDocument1,394 pagesWorld of Cultivationxdmhundz999No ratings yet
- The Trembling WorldDocument239 pagesThe Trembling Worldxdmhundz999No ratings yet
- 8the Experimental Log of A Crazy Lich (Fin)Document321 pages8the Experimental Log of A Crazy Lich (Fin)xdmhundz999No ratings yet
- 9emperor's Domination (Fin)Document879 pages9emperor's Domination (Fin)xdmhundz999No ratings yet
- Secretary LeoncioDocument3 pagesSecretary Leoncioxdmhundz999No ratings yet
- Galactic Dark NetDocument801 pagesGalactic Dark Netxdmhundz9990% (1)
- 8the Experimental Log of A Crazy Lich (Fin)Document321 pages8the Experimental Log of A Crazy Lich (Fin)xdmhundz999No ratings yet
- Gob TenseiDocument110 pagesGob Tenseixdmhundz999No ratings yet
- 2return of The Former Hero (Fin)Document306 pages2return of The Former Hero (Fin)xdmhundz999No ratings yet
- 9emperor's Domination (Fin)Document879 pages9emperor's Domination (Fin)xdmhundz999No ratings yet
- 9emperor's Domination (Fin)Document879 pages9emperor's Domination (Fin)xdmhundz999No ratings yet
- 6hokuou Kizoku To Moukinzuma No Yukiguni Karigurashi (Fin)Document281 pages6hokuou Kizoku To Moukinzuma No Yukiguni Karigurashi (Fin)xdmhundz9990% (1)
- DO s2016 47 PDFDocument55 pagesDO s2016 47 PDFxdmhundz999No ratings yet
- Punong Barangay Certification (PBC) : (For Barangay Check Disbursement)Document2 pagesPunong Barangay Certification (PBC) : (For Barangay Check Disbursement)xdmhundz999No ratings yet
- FILM SHOWING - August 29, 2015: Report On Pa-RaffleDocument2 pagesFILM SHOWING - August 29, 2015: Report On Pa-Rafflexdmhundz999No ratings yet
- FrontDocument2 pagesFrontxdmhundz999No ratings yet
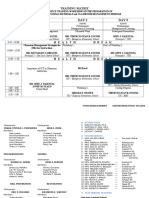
- Time Day 1 Day 2 Day 3: Training MatrixDocument3 pagesTime Day 1 Day 2 Day 3: Training Matrixxdmhundz999No ratings yet
- 2550Q FOrmDocument1 page2550Q FOrmxdmhundz999No ratings yet
- IBC and BCDocument2 pagesIBC and BCxdmhundz999No ratings yet
- 2015 Passers MidwifeDocument26 pages2015 Passers Midwifexdmhundz999No ratings yet