You might also like
- Pediatric Rehabilitation&geriatriDocument74 pagesPediatric Rehabilitation&geriatriLIEBERKHUNNo ratings yet
- Lesson-3 Infancy and Toddlerhood PDFDocument66 pagesLesson-3 Infancy and Toddlerhood PDFchat gazaNo ratings yet
- Pediatric Medical RehabilitationDocument74 pagesPediatric Medical Rehabilitationlilis lestariNo ratings yet
- Premature BabyDocument41 pagesPremature BabyVijith.V.kumar100% (9)
- First Principles: How a small problem in early life creates havoc across time.From EverandFirst Principles: How a small problem in early life creates havoc across time.No ratings yet
- Prenatal DevelopmentDocument29 pagesPrenatal DevelopmentReymart MancaoNo ratings yet
- Persistence of Primitive Reflexes and Associated Motor Problems in Healthy Preschool ChildrenDocument7 pagesPersistence of Primitive Reflexes and Associated Motor Problems in Healthy Preschool ChildrenDiana SchlittlerNo ratings yet
- Development TestDocument18 pagesDevelopment TesthypsdreamerNo ratings yet
- NannyTraining Unit 5 Physical Development of ChildrenDocument18 pagesNannyTraining Unit 5 Physical Development of ChildrenKanavv BhallaNo ratings yet
- Assignment in Physical Sexual SelfDocument2 pagesAssignment in Physical Sexual SelfKiana Vren JermiaNo ratings yet
- Written Report PsychDocument17 pagesWritten Report PsychShanaia BualNo ratings yet
- Principles of Motor DevelopmentDocument15 pagesPrinciples of Motor DevelopmentRina Siason AbaNo ratings yet
- Neuropediatric ExaminationDocument43 pagesNeuropediatric ExaminationShaniaNo ratings yet
- Stages of Human Growth & Development Prenatal Perinatal PostnatalDocument4 pagesStages of Human Growth & Development Prenatal Perinatal PostnatalameerabestNo ratings yet
- Gynecology AbnormalPubertyandGrowthProblemsDocument6 pagesGynecology AbnormalPubertyandGrowthProblemsBhi-An BatobalonosNo ratings yet
- Solve Your Child's Sleep Problems: Revised Edition: New, Revised, and Expanded EditionFrom EverandSolve Your Child's Sleep Problems: Revised Edition: New, Revised, and Expanded EditionRating: 4 out of 5 stars4/5 (19)
- Neonatal and Infancy PeriodDocument10 pagesNeonatal and Infancy PeriodJoji Santa MariaNo ratings yet
- Intro To Psych L3Document12 pagesIntro To Psych L3Abigail MorfeNo ratings yet
- Lecture 76 Growth, Development and Assessment of Newborns and ChildrenDocument75 pagesLecture 76 Growth, Development and Assessment of Newborns and ChildrenHeeb WardaNo ratings yet
- Module 3. Stages of Human Development: at The End of This Module, You Will Be Able ToDocument7 pagesModule 3. Stages of Human Development: at The End of This Module, You Will Be Able ToRheamar Angel MolinaNo ratings yet
- Adolescence and Adulthood 1Document17 pagesAdolescence and Adulthood 1Shyica SalacNo ratings yet
- Reaching The Age of AdolesenceDocument7 pagesReaching The Age of Adolesencestarprintout23No ratings yet
- The Good Night Sleep Tight Workbook for Children Special Needs: Gentle Proven Solutions to Help Your Child with Exceptional Needs Sleep WellFrom EverandThe Good Night Sleep Tight Workbook for Children Special Needs: Gentle Proven Solutions to Help Your Child with Exceptional Needs Sleep WellRating: 5 out of 5 stars5/5 (1)
- 9 Developmental Lecture NotesDocument33 pages9 Developmental Lecture NotesReseNo ratings yet
- Week 7 Devt - StudentDocument7 pagesWeek 7 Devt - StudentSamer FarhanNo ratings yet
- Summary of Dirty Genes: by Ben Lynch ND. - A Breakthrough Program to Treat the Root Cause of Illness and Optimize Your Health - A Comprehensive SummaryFrom EverandSummary of Dirty Genes: by Ben Lynch ND. - A Breakthrough Program to Treat the Root Cause of Illness and Optimize Your Health - A Comprehensive SummaryNo ratings yet
- Baby Sleep Training Book:What Works (And What Your Grandparents Forgot to Tell You)From EverandBaby Sleep Training Book:What Works (And What Your Grandparents Forgot to Tell You)No ratings yet
- What Is Child PsychologyDocument16 pagesWhat Is Child PsychologyTalha MughalNo ratings yet
- Psychology 1000 Notes (Chapters 9-17)Document6 pagesPsychology 1000 Notes (Chapters 9-17)Ninth ExplorerNo ratings yet
- Theories Relevant To Nursing PracticeDocument61 pagesTheories Relevant To Nursing PracticeAngel BarrocaNo ratings yet
- Daddy Happiness Ahoy: All about pregnancy, birth, breastfeeding, hospital bag, baby equipment and baby sleep! (Pregnancy guide for expectant parents)From EverandDaddy Happiness Ahoy: All about pregnancy, birth, breastfeeding, hospital bag, baby equipment and baby sleep! (Pregnancy guide for expectant parents)Rating: 5 out of 5 stars5/5 (10)
- Chapter 8 Human DVLP Part 1Document40 pagesChapter 8 Human DVLP Part 1Isha KanojiaNo ratings yet
- 5 - Paed ReflexesDocument41 pages5 - Paed Reflexesmemoona kaleemNo ratings yet
- Human Biology: Sixth GradeDocument25 pagesHuman Biology: Sixth GradeJohn DeHansNo ratings yet
- Developmental Psychology PPDocument159 pagesDevelopmental Psychology PPMarce BustamanteNo ratings yet
- 6.1 Assessment of Fetal Growth & DevekiomentDocument9 pages6.1 Assessment of Fetal Growth & DevekiomentRafael OliveiraNo ratings yet
- Stages of Development and Developmental TasksDocument6 pagesStages of Development and Developmental TasksJeyd Montefalco100% (1)
- Arun Thachil BPT, MPT (Ortho) : PhysiotherapistDocument56 pagesArun Thachil BPT, MPT (Ortho) : PhysiotherapistDeepa SeiraNo ratings yet
- How To Have an Easy and Safe Pregnancy and Bring Forth a Healthy Baby: A Pregnancy Book for First Time Moms for a Successful and Healthy Journey through Pregnancy, Childbirth and NewbornFrom EverandHow To Have an Easy and Safe Pregnancy and Bring Forth a Healthy Baby: A Pregnancy Book for First Time Moms for a Successful and Healthy Journey through Pregnancy, Childbirth and NewbornNo ratings yet
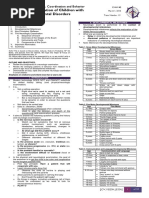
- Neurologic Evaluation of Children With Neurodevelopmental DisordersDocument10 pagesNeurologic Evaluation of Children With Neurodevelopmental DisordersAthan AntonioNo ratings yet
- Teaching Tools For ParentsDocument14 pagesTeaching Tools For Parentsapi-458854276No ratings yet
- Sleep Routines for Baby and You: How to Help Your Child Sleep Through the Night and Finally Get the Rest You Crave (From Newborn to School Age)From EverandSleep Routines for Baby and You: How to Help Your Child Sleep Through the Night and Finally Get the Rest You Crave (From Newborn to School Age)No ratings yet
- Infant ReflexesDocument41 pagesInfant ReflexesamwriteaNo ratings yet
- Iv. The Physical SelfDocument7 pagesIv. The Physical SelfEddie MunsonNo ratings yet
- Sexual SelfDocument35 pagesSexual SelfMatet GenerosaNo ratings yet
- Sexual Behavior and Teens - Community PresentationDocument55 pagesSexual Behavior and Teens - Community PresentationAfreen Kamal100% (1)
- Growth and Development of ChildrenDocument108 pagesGrowth and Development of Childrenabdisalaan hassanNo ratings yet
- Unit Iv Chapter Vi Chapter Vii Dev PsychDocument27 pagesUnit Iv Chapter Vi Chapter Vii Dev PsychAsteann Alexandra VillalonNo ratings yet
- PDF DocumentDocument54 pagesPDF DocumentMLS1B-NAVAREZ, MA. JULIET LOURDESNo ratings yet
- Attention, Balance and Coordination: The A.B.C. of Learning SuccessFrom EverandAttention, Balance and Coordination: The A.B.C. of Learning SuccessNo ratings yet
- Autism B Theory: The Cause, Development and Support of AutismFrom EverandAutism B Theory: The Cause, Development and Support of AutismNo ratings yet
- Neurodevelopmental Therapy Inhibition of Primitive ReflexesDocument11 pagesNeurodevelopmental Therapy Inhibition of Primitive ReflexesZoran Constantinescu80% (5)
- 10: Physical Development: Student ObjectivesDocument9 pages10: Physical Development: Student ObjectivesŞterbeţ RuxandraNo ratings yet
- 3 - Human DevelopmentDocument12 pages3 - Human DevelopmentAnonymous 6p4hve4No ratings yet
- Unit 4 Pies and InfancyDocument31 pagesUnit 4 Pies and Infancyapi-200177496No ratings yet
- 5pediatrics2.1 Neuro Exam Uerm2015bDocument6 pages5pediatrics2.1 Neuro Exam Uerm2015bbeia21No ratings yet
- Growing up Book for Boys: Becoming a Teen , Skin Care and Guys StuffFrom EverandGrowing up Book for Boys: Becoming a Teen , Skin Care and Guys StuffNo ratings yet
- Developmental PsychologyDocument30 pagesDevelopmental PsychologyLeizel Fajardo - Metillo100% (1)
- Modified ILOA FormDocument1 pageModified ILOA FormRoger100% (1)
- Neurodynamic Technique Practice: Spine, Cord and MeningesDocument14 pagesNeurodynamic Technique Practice: Spine, Cord and MeningesRogerNo ratings yet
- Rehabilitation of Patients After StrokeDocument47 pagesRehabilitation of Patients After StrokeRogerNo ratings yet
- Fall Risk Screen TugDocument2 pagesFall Risk Screen TugRogerNo ratings yet
- Duchenne Muscular DystrophyDocument27 pagesDuchenne Muscular DystrophyRogerNo ratings yet
- Clinical PediatricDocument214 pagesClinical PediatricRogerNo ratings yet