You might also like
- Usps Form 1583Document3 pagesUsps Form 1583Strav Rosemond100% (2)
- 1040 Exam Prep: Module II - Basic Tax ConceptsFrom Everand1040 Exam Prep: Module II - Basic Tax ConceptsRating: 1.5 out of 5 stars1.5/5 (2)
- Form1583 PDFDocument3 pagesForm1583 PDFJorrell LawtonNo ratings yet
- Form 1583Document2 pagesForm 1583Eduardo LimaNo ratings yet
- Form 1583Document1 pageForm 1583Stalin GarciaNo ratings yet
- Formula Rio 14886Document1 pageFormula Rio 14886Nuñez Fonseca JoseNo ratings yet
- USPS Form 1583 BlaineDocument2 pagesUSPS Form 1583 BlaineKate GrayNo ratings yet
- Ps 1583 NDocument2 pagesPs 1583 NMark BogumilNo ratings yet
- Form 1583Document3 pagesForm 1583Steven SmithNo ratings yet
- Form 1583Document2 pagesForm 1583Theplaymaker508No ratings yet
- Application For Delivery of Mail Through Agent: See Privacy Act Statement On ReverseDocument2 pagesApplication For Delivery of Mail Through Agent: See Privacy Act Statement On ReverseAnonymous 5PYmqgCXzrNo ratings yet
- What To Do Next: Khalid KazyDocument3 pagesWhat To Do Next: Khalid KazyKhalid QaziNo ratings yet
- Form 1583 FLDocument2 pagesForm 1583 FLerichfriedmanNo ratings yet
- Attention:: Order Information Returns and Employer Returns OnlineDocument6 pagesAttention:: Order Information Returns and Employer Returns OnlineIRSNo ratings yet
- 4506 TDocument3 pages4506 Tteddy rooseveltNo ratings yet
- W-9 Tax FormDocument4 pagesW-9 Tax FormMika DjokaNo ratings yet
- bmv2424 PDFDocument2 pagesbmv2424 PDFAli AldosNo ratings yet
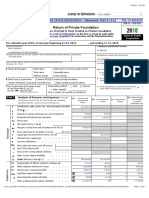
- 2018 NoVo 990Document80 pages2018 NoVo 990Noam Blum100% (1)
- 4506 TDocument3 pages4506 TwallerdcNo ratings yet
- How To Apply P-EBTDocument2 pagesHow To Apply P-EBTMorgan BurrellNo ratings yet
- Assumed Name IndividualDocument1 pageAssumed Name IndividualShiv Raj MathurNo ratings yet
- Classification Election. See Form 8832 and Its Instructions For Additional InformationDocument3 pagesClassification Election. See Form 8832 and Its Instructions For Additional Informationдиковець пашаNo ratings yet
- Annual Return To Report Transactions With Foreign Trusts and Receipt of Certain Foreign GiftsDocument1 pageAnnual Return To Report Transactions With Foreign Trusts and Receipt of Certain Foreign GiftsCarolina AldanaNo ratings yet
- 1099 Misc 1Document1 page1099 Misc 1Anonymous FR8yGDSVgNo ratings yet
- Business License Application-1Document5 pagesBusiness License Application-1Keller Brown JnrNo ratings yet
- IRS E-File Signature AuthorizationDocument2 pagesIRS E-File Signature AuthorizationKatia AlvezNo ratings yet
- Ve'H (O5.U H + Q ": Frlitf (TFF Califi ,,'R? Q L (O?ODocument1 pageVe'H (O5.U H + Q ": Frlitf (TFF Califi ,,'R? Q L (O?OMatthew Robert QuinnNo ratings yet
- Taxpayer Identification RequestDocument1 pageTaxpayer Identification RequestmoNo ratings yet
- Certificate of Ownership Template 11Document1 pageCertificate of Ownership Template 11RichardwilsonNo ratings yet
- Articles of Incorporation NY Dos1511Document4 pagesArticles of Incorporation NY Dos1511asdfpoiuiiiiNo ratings yet
- W9 FormDocument1 pageW9 FormChris GreeneNo ratings yet
- Articles of Incorporation MainstreetDocument8 pagesArticles of Incorporation MainstreetSophia PeronNo ratings yet
- Illinois State Police - FOID ApplicationDocument2 pagesIllinois State Police - FOID ApplicationrhippleNo ratings yet
- Tda1086 PDFDocument15 pagesTda1086 PDFmsb.raNo ratings yet
- Certificate of Baptism: This Certifies ThatDocument1 pageCertificate of Baptism: This Certifies ThatJinsen Paul MartinNo ratings yet
- Acceptance of Appointment and OathDocument2 pagesAcceptance of Appointment and OathMinnesota Public RadioNo ratings yet
- Trade NameDocument3 pagesTrade Namerene andre smithNo ratings yet
- ds5504 PDFDocument6 pagesds5504 PDFAnonymous Rrs8EyL100% (1)
- If You Need Help Reading or Completing This Document or Need Help Communicating With Us, Ask Us orDocument19 pagesIf You Need Help Reading or Completing This Document or Need Help Communicating With Us, Ask Us ordavid rawlinsNo ratings yet
- BMI-Africa IRS EIN #Document3 pagesBMI-Africa IRS EIN #Joseph VillarosaNo ratings yet
- CP575 1372187182568Document3 pagesCP575 1372187182568vinie davisNo ratings yet
- Missouri LLC Articles of OrganizationDocument4 pagesMissouri LLC Articles of OrganizationRocketLawyer100% (1)
- Sec Form 4Document1 pageSec Form 4Nick WeigNo ratings yet
- State - Form - 49607 Application Birth CertificateDocument1 pageState - Form - 49607 Application Birth CertificateLINDANo ratings yet
- Articles of AssociationDocument2 pagesArticles of AssociationMadan MathodNo ratings yet
- Approved Ein - FS Ventures IncDocument3 pagesApproved Ein - FS Ventures IncKarthi KeyanNo ratings yet
- Current I-9 FormDocument4 pagesCurrent I-9 Formlegiziano100% (4)
- Form 1583Document2 pagesForm 1583LukmanNo ratings yet
- Ps 1583Document2 pagesPs 1583api-256669606No ratings yet
- Nortarize Form-UpdateDocument4 pagesNortarize Form-Updatewaqar chNo ratings yet
- Instructions For USPS Form 1583Document3 pagesInstructions For USPS Form 1583kewtashNo ratings yet
- Instructions For USPS Form 1583Document3 pagesInstructions For USPS Form 1583Dan LeeNo ratings yet
- Form1583 Virtual MailDocument3 pagesForm1583 Virtual MailEnrique Berrocal SalazarNo ratings yet
- Form 1583Document3 pagesForm 1583Jose Vicente Bolivar DazaNo ratings yet
- PS 1583 Form SampleDocument1 pagePS 1583 Form SampleFenellaNo ratings yet
- ps1583 PDFDocument3 pagesps1583 PDFowen tsangNo ratings yet
- Application For Delivery of Mail Through Agent: # - 1 Aeropost Way / P.O. BOX MiamiDocument1 pageApplication For Delivery of Mail Through Agent: # - 1 Aeropost Way / P.O. BOX MiamiAlex Gerson Perez RojasNo ratings yet
- Planilla Usps Venezuela PDFDocument1 pagePlanilla Usps Venezuela PDFAdriana VargasNo ratings yet
- Application For Delivery of Mail Through Agent: 2240 N.W., 114th Ave., Unit ZMDocument1 pageApplication For Delivery of Mail Through Agent: 2240 N.W., 114th Ave., Unit ZMNinibeth Zamora AguilarNo ratings yet
- April 13, 2016Document16 pagesApril 13, 2016The Delphos HeraldNo ratings yet
- Ship ShapesDocument18 pagesShip ShapeszaamanishNo ratings yet
- Tim Turner Freedom Seminar Documents CD - Section 3Document19 pagesTim Turner Freedom Seminar Documents CD - Section 3YoPatrona100% (6)
- An Overview of Post OfficeDocument57 pagesAn Overview of Post OfficezendilaNo ratings yet
- Non Domestic Mail Postage 2 CentsDocument2 pagesNon Domestic Mail Postage 2 Centsbind1967100% (8)
- Woodsmith No. 252 - Vol. 42 - Diciembre-Enero 2021Document70 pagesWoodsmith No. 252 - Vol. 42 - Diciembre-Enero 2021rpreciadoruizNo ratings yet
- Usps 708Document56 pagesUsps 708trujillo66@yahooNo ratings yet
- Architect AIA Magazine 2021 11 12Document104 pagesArchitect AIA Magazine 2021 11 12Marco Milazzo100% (1)
- Indian Post - Startegic PlanDocument33 pagesIndian Post - Startegic PlanChandraMohan GargNo ratings yet
- Wells Fargo Everyday Checking: Important Account InformationDocument4 pagesWells Fargo Everyday Checking: Important Account InformationWillian FinchNo ratings yet
- Qdoc - Tips - B00pwe81ve Strategic Storytelling PDFDocument161 pagesQdoc - Tips - B00pwe81ve Strategic Storytelling PDFAcosta ManuelNo ratings yet
- WISP Marketing Tips To Grow Your BusinessDocument20 pagesWISP Marketing Tips To Grow Your BusinessMarcos Baylosis JrNo ratings yet
- Cover LetterDocument19 pagesCover LetterAhmed M AminNo ratings yet
- Instructions Online Label Record: Usps Tracking #Document1 pageInstructions Online Label Record: Usps Tracking #Ernesto PadronNo ratings yet
- 240 Popular Woodworking 08-2018Document66 pages240 Popular Woodworking 08-2018NobodyXX66No ratings yet
- Commercial Dispatch Eedition 10-13-19Document28 pagesCommercial Dispatch Eedition 10-13-19The DispatchNo ratings yet
- Bluecrest - Mail-Mailstream Evolution Equipment Schedule A and BDocument6 pagesBluecrest - Mail-Mailstream Evolution Equipment Schedule A and BPaul WallNo ratings yet
- Updated Terms and Conditionals 11-30-2021Document7 pagesUpdated Terms and Conditionals 11-30-2021api-577083134No ratings yet
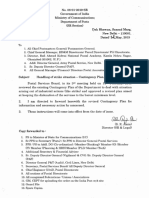
- Contingency Plan - Letter No. 08-01-2019-SR Dated 03-05-2019 - 19 PagesDocument19 pagesContingency Plan - Letter No. 08-01-2019-SR Dated 03-05-2019 - 19 PageshemanthpeekaNo ratings yet
- Commercial Dispatch Eedition 11-5-18Document12 pagesCommercial Dispatch Eedition 11-5-18The DispatchNo ratings yet
- "Barcode" Web Service: ManualDocument64 pages"Barcode" Web Service: ManualЕгон ЧарнојевићNo ratings yet
- Starkville Dispatch Eedition 8-13-17Document28 pagesStarkville Dispatch Eedition 8-13-17The DispatchNo ratings yet
- MBA Acceptance Letters OpsDocument14 pagesMBA Acceptance Letters OpsAtul Anand bj21135No ratings yet
- Philippine Education Co. Inc. v. SorianoDocument7 pagesPhilippine Education Co. Inc. v. SorianoBLACK mambaNo ratings yet
- Steps in Handling MailDocument9 pagesSteps in Handling MailJerome MakaNo ratings yet
- Common Questions About Post Office ClosuresDocument15 pagesCommon Questions About Post Office ClosuresbsheehanNo ratings yet
- Customer Service Templates (CS)Document12 pagesCustomer Service Templates (CS)said ObnikaNo ratings yet
- Blue Border Offset and Indemnity Bond 10-03-08Document5 pagesBlue Border Offset and Indemnity Bond 10-03-08Michael Nguyen Thornton92% (12)
- Elevate Invoice CivisDocument1 pageElevate Invoice CivisRob LauciusNo ratings yet
- USPS Change of AddressDocument20 pagesUSPS Change of AddressmegcorNo ratings yet