You might also like
- MedicalcertificateDocument1 pageMedicalcertificateDessa Ruth ReyesNo ratings yet
- NBS & Discharge Plan (New)Document3 pagesNBS & Discharge Plan (New)Aina HaravataNo ratings yet
- Next Gen Med ReleaseDocument2 pagesNext Gen Med ReleaserfbcgreenvilleNo ratings yet
- Registration and Consent 2013-2014Document2 pagesRegistration and Consent 2013-2014Fiona WilliamsNo ratings yet
- Philippine Obstetrical and Gynecological Society (Foundation), Inc Philippine Board of Obstetrics and GynecologyDocument2 pagesPhilippine Obstetrical and Gynecological Society (Foundation), Inc Philippine Board of Obstetrics and GynecologyThor Jan AustriaNo ratings yet
- Satellite Communications DefinitionsDocument1 pageSatellite Communications DefinitionsGuillenvincent E FranNo ratings yet
- Patient Information: X - Patient Signature or Legal Representative DateDocument1 pagePatient Information: X - Patient Signature or Legal Representative DateJohn FrinkNo ratings yet
- Health Examination CardDocument2 pagesHealth Examination Cardサシンゴ ラアーニNo ratings yet
- Parents Consent 2023Document2 pagesParents Consent 2023danosoprince39No ratings yet
- 2014 Alc Short Term Missions Team ApplicationDocument5 pages2014 Alc Short Term Missions Team Applicationapi-254122285No ratings yet
- Cues Nursing Diagnosis Scientific Explanation Nursing Objective Nursing Intervention Scientific Explanation EvaluationDocument2 pagesCues Nursing Diagnosis Scientific Explanation Nursing Objective Nursing Intervention Scientific Explanation EvaluationJessa BorreNo ratings yet
- ApplicationDocument2 pagesApplicationMark McCoyNo ratings yet
- COMPANY NAME: - Regular Salaried Employees - 18 To 65 Years OldDocument1 pageCOMPANY NAME: - Regular Salaried Employees - 18 To 65 Years OldCart Sunrise AguillonNo ratings yet
- Health Statement FormDocument1 pageHealth Statement FormALT IkedaNo ratings yet
- Admission Agreement Health AssessmentDocument2 pagesAdmission Agreement Health AssessmentweewolvesNo ratings yet
- COVID 19 Revised Monitoring Form 2021Document3 pagesCOVID 19 Revised Monitoring Form 2021Aaron Paul BernasNo ratings yet
- Student Profile Form For Inventory - PDFDocument2 pagesStudent Profile Form For Inventory - PDFLeen Ganoran100% (1)
- Registration 2010 2011Document3 pagesRegistration 2010 2011cubanita11No ratings yet
- Fhel Anthony V. Ubalde: Upper Musi-Musi, Blanco, Balingasag, Misamis OrientalDocument3 pagesFhel Anthony V. Ubalde: Upper Musi-Musi, Blanco, Balingasag, Misamis OrientalDanniNo ratings yet
- Antipolo City Senior High School District I-A: Last Menstruation Period: - (For Girls Only)Document2 pagesAntipolo City Senior High School District I-A: Last Menstruation Period: - (For Girls Only)Chlong ArtuzNo ratings yet
- San Vicente Ferrer Chapel Kibleg, Upi, Maguindanao: To Whom It May ConcernDocument2 pagesSan Vicente Ferrer Chapel Kibleg, Upi, Maguindanao: To Whom It May ConcernOnjhong FaeldenNo ratings yet
- Proxy FormDocument1 pageProxy FormSarahNo ratings yet
- Camping Health, Consent and Release FormDocument4 pagesCamping Health, Consent and Release FormJohn PowellNo ratings yet
- Pahintulot para Sa Day Care ServiceDocument9 pagesPahintulot para Sa Day Care ServiceKathleen Rose LibedNo ratings yet
- Brown Hearing Centers: Personal InformationDocument2 pagesBrown Hearing Centers: Personal InformationEddie TooheyNo ratings yet
- Medical Certificate23Document1 pageMedical Certificate23Donna Karen MoronNo ratings yet
- Antenatal Booking Visit FormDocument4 pagesAntenatal Booking Visit FormAnanya Kruthika PalapartiNo ratings yet
- Ms 2083 EngDocument1 pageMs 2083 Engapi-509258857No ratings yet
- BHW Monthly ReportDocument2 pagesBHW Monthly Reportsucuanojoan199No ratings yet
- Pregnant Female AssesmentDocument4 pagesPregnant Female AssesmentJenNo ratings yet
- Registration FormDocument1 pageRegistration Formbobbelmiasco25No ratings yet
- OSCA ID Application For Senior CitizenDocument2 pagesOSCA ID Application For Senior Citizenbarangay twentynineNo ratings yet
- Nutritional Clinical History Pregnant WomanDocument13 pagesNutritional Clinical History Pregnant WomanScribdTranslationsNo ratings yet
- CertificateofhealthDocument1 pageCertificateofhealthlolalelaNo ratings yet
- Medical FormDocument1 pageMedical Formapi-144496227No ratings yet
- Faith Formation Registration Form: St. Joachim Catholic Church, 900 W. Broadway, Plainview, MN 55964Document1 pageFaith Formation Registration Form: St. Joachim Catholic Church, 900 W. Broadway, Plainview, MN 55964saintjoachimdffNo ratings yet
- Cuidados Posoperatorio CirugiaDocument1 pageCuidados Posoperatorio CirugiaAna CristernaNo ratings yet
- Summer Events - Consent FormDocument3 pagesSummer Events - Consent FormKeon Gunie HuhNo ratings yet
- Teen MedicalDocument1 pageTeen MedicalJohn C StarkNo ratings yet
- FC Child-Adolescent Intake Forms Fisa AdolescentDocument4 pagesFC Child-Adolescent Intake Forms Fisa Adolescentnicoletagr2744No ratings yet
- WOW Kid's Club Health FormDocument4 pagesWOW Kid's Club Health FormKetron Memorial United Methodist ChurchNo ratings yet
- Phlebotomy Tech FormDocument4 pagesPhlebotomy Tech FormHawaiiHealthCareNo ratings yet
- Patient Entrance Form1 2019 12ptpdfDocument6 pagesPatient Entrance Form1 2019 12ptpdfapi-478211107No ratings yet
- FORM B - Physical - STUDENTDocument4 pagesFORM B - Physical - STUDENTJane PNo ratings yet
- Health Medical QuestionaireDocument1 pageHealth Medical QuestionaireALT IkedaNo ratings yet
- Sworn StatementDocument1 pageSworn StatementHannah Ben AragonNo ratings yet
- Sworn Statement: IN WITNESS WHEREOF, I Have Hereunto Set My Hand ThisDocument1 pageSworn Statement: IN WITNESS WHEREOF, I Have Hereunto Set My Hand ThisJessie Montes JrNo ratings yet
- Sworn Statement For Public EmployeesDocument1 pageSworn Statement For Public EmployeesAngie BasconesNo ratings yet
- 2018 Sworn Statement 1Document1 page2018 Sworn Statement 1Phebe Zhie Zhia CampeñaNo ratings yet
- Newborn-Infirmation SheetDocument7 pagesNewborn-Infirmation SheetJONABELL B YLAGANNo ratings yet
- New Client Questionnaire 12-28-2011Document7 pagesNew Client Questionnaire 12-28-2011api-234610379No ratings yet
- Registration Form 0-3.8 YearsDocument2 pagesRegistration Form 0-3.8 YearsJackson SilvaNo ratings yet
- Alabama Advance Directive For Health Care: Section I - Living WillDocument5 pagesAlabama Advance Directive For Health Care: Section I - Living WillKilluaNo ratings yet
- Acetaminphen Drug StudyDocument2 pagesAcetaminphen Drug StudymilesminNo ratings yet
- New Patient FormDocument8 pagesNew Patient Forme-MedTools100% (5)
- DMSF College of Medicine ApplicationDocument4 pagesDMSF College of Medicine ApplicationJehannaMarEnggingAbdurahmanNo ratings yet
- Submit This Application To Your Church LeadershipDocument4 pagesSubmit This Application To Your Church LeadershiparobinwaNo ratings yet
- Certificate of Physical Fitness: IA. History of Any Known Illness / SurgeryDocument5 pagesCertificate of Physical Fitness: IA. History of Any Known Illness / SurgeryPrakash RNo ratings yet
- Republic of The Philippines Department of Education Region V-Bicol Schools Division Office of AlbayDocument3 pagesRepublic of The Philippines Department of Education Region V-Bicol Schools Division Office of AlbayDexter Rabo100% (1)
- Blended Learning RBI and Modular Subject Schedule Week 1 4 1Document4 pagesBlended Learning RBI and Modular Subject Schedule Week 1 4 1Dexter RaboNo ratings yet
- Lesson PlanDocument4 pagesLesson PlanDexter RaboNo ratings yet
- ST 2 - English 6 - Q1Document1 pageST 2 - English 6 - Q1Dexter RaboNo ratings yet
- DALOGO ES - Revised-SBM-Assessment-Tool-Validation-Form-FINAL - 1Document14 pagesDALOGO ES - Revised-SBM-Assessment-Tool-Validation-Form-FINAL - 1Dexter RaboNo ratings yet
- Spore Bearing and Cone Bearing Plants - Docx Version 1Document2 pagesSpore Bearing and Cone Bearing Plants - Docx Version 1Dexter Rabo100% (1)
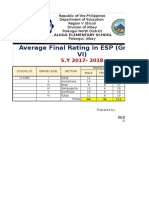
- DALOGO ES - Average Final Rating in ESP VIDocument2 pagesDALOGO ES - Average Final Rating in ESP VIDexter RaboNo ratings yet
- Dalogo CERTIFICATION 2018Document1 pageDalogo CERTIFICATION 2018Dexter RaboNo ratings yet
- Data Submission Template On The Diff Trainings On K To 12 LDPDocument6 pagesData Submission Template On The Diff Trainings On K To 12 LDPDexter RaboNo ratings yet
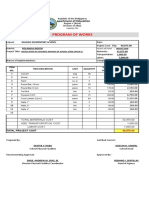
- Program of WORK 2018Document5 pagesProgram of WORK 2018Dexter RaboNo ratings yet
- IPCRF Transmittal (Dalogo)Document2 pagesIPCRF Transmittal (Dalogo)Dexter RaboNo ratings yet
- Brigada Eskwela 2016: Narrative ReportDocument2 pagesBrigada Eskwela 2016: Narrative ReportDexter RaboNo ratings yet
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesDexter RaboNo ratings yet
- Quarter 1 Project Monitoring Report FormDocument1 pageQuarter 1 Project Monitoring Report FormDexter RaboNo ratings yet
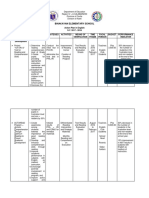
- Action Plan in English2016 2017Document6 pagesAction Plan in English2016 2017Dexter Rabo100% (2)
- Letter To Guest SpeakerDocument1 pageLetter To Guest SpeakerDexter Rabo86% (7)
- Certification: Polangui North DistrictDocument3 pagesCertification: Polangui North DistrictDexter RaboNo ratings yet
- Department of Education: Candidates For Master and Miss Yuletide 2017Document2 pagesDepartment of Education: Candidates For Master and Miss Yuletide 2017Dexter RaboNo ratings yet
- Department of Education: Republic of The PhilippinesDocument1 pageDepartment of Education: Republic of The PhilippinesDexter RaboNo ratings yet
- Department of Education: Dalogo Elementary SchoolDocument4 pagesDepartment of Education: Dalogo Elementary SchoolDexter RaboNo ratings yet
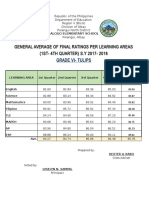
- General Average of Final Ratings Per Learning Areas (1ST-4TH QUARTER) S.Y 2017 - 2018Document1 pageGeneral Average of Final Ratings Per Learning Areas (1ST-4TH QUARTER) S.Y 2017 - 2018Dexter RaboNo ratings yet