You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- V&VR PDFDocument199 pagesV&VR PDFTalbain100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Template, Yo: Praesent Congue Sapien Sit Amet Justo. VivamusDocument2 pagesTemplate, Yo: Praesent Congue Sapien Sit Amet Justo. VivamusthatshipcreighNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Respiration Physiology SEQs With KeyDocument12 pagesRespiration Physiology SEQs With KeyMudassar Roomi100% (1)
- List of Greek and Latin Roots in English PDFDocument39 pagesList of Greek and Latin Roots in English PDFMvrnaidu MithraNo ratings yet
- Ectopic PregnancyDocument78 pagesEctopic PregnancyCarie Manarondong80% (5)
- Rip Autopsy ReportDocument4 pagesRip Autopsy Reportapi-397001333No ratings yet
- White Coat BooksDocument2 pagesWhite Coat BooksthatshipcreighNo ratings yet
- Q 1MCQs Microbiology For MRCP and MRCPathDocument40 pagesQ 1MCQs Microbiology For MRCP and MRCPathDr Sumant SharmaNo ratings yet
- Donald Marshall. Volume 1. Experiences From The Cloning Centre April 5th 2012 - May 18th 2012Document37 pagesDonald Marshall. Volume 1. Experiences From The Cloning Centre April 5th 2012 - May 18th 2012Gold EnTruthNo ratings yet
- Case Presentation On CVTDocument32 pagesCase Presentation On CVTraman kumariNo ratings yet
- SCRIBD'edDocument2 pagesSCRIBD'edthatshipcreighNo ratings yet
- I Think This Is How Scribd Works: Test Tes 1,2Document1 pageI Think This Is How Scribd Works: Test Tes 1,2thatshipcreighNo ratings yet
- Internal Medicine Clerkship AdviceDocument2 pagesInternal Medicine Clerkship AdvicethatshipcreighNo ratings yet
- Not Sure How This WorksDocument1 pageNot Sure How This WorksthatshipcreighNo ratings yet
- Scribd Test 12Document1 pageScribd Test 12thatshipcreighNo ratings yet
- Scribd Test 8: I'm Still Not Sure How This Works Part DosDocument1 pageScribd Test 8: I'm Still Not Sure How This Works Part DosthatshipcreighNo ratings yet
- Scribd Test 10Document1 pageScribd Test 10thatshipcreighNo ratings yet
- Scribd Test 11Document1 pageScribd Test 11thatshipcreighNo ratings yet
- Scribd Test 9: I'm Still Not Sure How This Works Part DosDocument1 pageScribd Test 9: I'm Still Not Sure How This Works Part DosthatshipcreighNo ratings yet
- Scribd Test 7: I'm Still Not Sure How This Works Part DosDocument1 pageScribd Test 7: I'm Still Not Sure How This Works Part DosthatshipcreighNo ratings yet
- Scribd Test 6: I'm Still Not Sure How This Works Part DosDocument1 pageScribd Test 6: I'm Still Not Sure How This Works Part DosthatshipcreighNo ratings yet
- Antibiotics 9Document11 pagesAntibiotics 9Beth Morales100% (1)
- Pogil Ecological RelationshipsDocument8 pagesPogil Ecological Relationshipsapi-3696769900% (1)
- Structure and Functions of The Skelital SystemDocument6 pagesStructure and Functions of The Skelital SystemLucshaan GaneshadasanNo ratings yet
- Presentation of DR Ishwar Gilada of AIDS Society of India in World AIDS Day 2016 WebinarDocument29 pagesPresentation of DR Ishwar Gilada of AIDS Society of India in World AIDS Day 2016 WebinarbobbyramakantNo ratings yet
- Dental Certificate 2010 PalaroDocument1 pageDental Certificate 2010 PalaroERDA BUENAFENo ratings yet
- Endocrine Function Test (Complete)Document79 pagesEndocrine Function Test (Complete)prayag mananiNo ratings yet
- Malabsorption Syndrome in ChickensDocument5 pagesMalabsorption Syndrome in ChickensŠhâh NawazNo ratings yet
- Fasting Can Save Your Life and Multiple SclerosisDocument3 pagesFasting Can Save Your Life and Multiple SclerosisJonas Sunshine Callewaert100% (1)
- PAEDIATRICS Notes 3 Update PDFDocument69 pagesPAEDIATRICS Notes 3 Update PDFMateen ShukriNo ratings yet
- Incubating Artificial Organs: David Rew 2/12/1Document16 pagesIncubating Artificial Organs: David Rew 2/12/1api-336220957No ratings yet
- Daftar Alat Dan Reagen BHPDocument12 pagesDaftar Alat Dan Reagen BHPCharles Bravo Alfredo MaitNo ratings yet
- Test5 Congenital MalformationDocument7 pagesTest5 Congenital MalformationDera Uzoaku OkekeNo ratings yet
- Literature Review On Pig Production in NigeriaDocument8 pagesLiterature Review On Pig Production in Nigeriac5hfb2ct100% (1)
- Animal Behavior ObservationDocument5 pagesAnimal Behavior ObservationRaúl AltamiranoNo ratings yet
- Blood Banking MT1ADocument10 pagesBlood Banking MT1ALeoPaulNo ratings yet
- Gigi Tiruan GasketDocument5 pagesGigi Tiruan GasketGus BasyaNo ratings yet
- 1 Introduction SymbiosisDocument229 pages1 Introduction Symbiosisbex9gg100% (1)
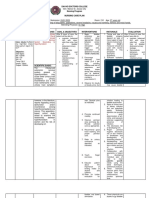
- Davao Doctors College Nursing Program Nursing Care PlanDocument3 pagesDavao Doctors College Nursing Program Nursing Care PlanPRINCESS KOBAYASHINo ratings yet
- BCG VaccinationDocument4 pagesBCG VaccinationOlive Health Travel ClinicNo ratings yet
- THE Lymphatic System & Body DefensesDocument39 pagesTHE Lymphatic System & Body DefensesSaiful AmriNo ratings yet
- Imle .20.09.2012Document39 pagesImle .20.09.2012Nas ManNo ratings yet
- ImunofarmakologiDocument63 pagesImunofarmakologiShafiraNo ratings yet