You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Addicted To Love - Jan GeurtzDocument20 pagesAddicted To Love - Jan GeurtzMariaelizaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Question Bank GOCDocument10 pagesQuestion Bank GOCAshutosh Tripathi100% (2)
- Cotton Pouches SpecificationsDocument2 pagesCotton Pouches SpecificationspunnareddytNo ratings yet
- Jan 08 Syn As ChemDocument20 pagesJan 08 Syn As ChemKetan PatelNo ratings yet
- Diabetic KetoacidosisDocument38 pagesDiabetic KetoacidosisEdelrose LapitanNo ratings yet
- Arlegui Seminar RoomDocument1 pageArlegui Seminar RoomGEMMA PEPITONo ratings yet
- E 6YI 7650-E: Thapar Institute of Engineering & Technology, PatialaDocument1 pageE 6YI 7650-E: Thapar Institute of Engineering & Technology, PatialaVaisnavi VNo ratings yet
- International Journal of Educational Research 103 (2020) 101634Document12 pagesInternational Journal of Educational Research 103 (2020) 101634Che Soh bin Said SaidNo ratings yet
- Gen. Chem. Module 1 PTDocument9 pagesGen. Chem. Module 1 PTjulianneNo ratings yet
- 1600 Bro enDocument2 pages1600 Bro enJenderalKancilNo ratings yet
- Abortion Op EdDocument3 pagesAbortion Op EdMadeline GlotfeltyNo ratings yet
- Transport of GasesDocument39 pagesTransport of GasesJayballabh KumarNo ratings yet
- Laboratory Associated Infections: Tania Chintya IKD BiomedikDocument16 pagesLaboratory Associated Infections: Tania Chintya IKD BiomedikTania Chintya Dewi KarimaNo ratings yet
- ASME17-1 - Wire Rope Replacement CriteriaDocument2 pagesASME17-1 - Wire Rope Replacement Criteriaegyinspectoryahoo100% (1)
- DG1 Installation Manual 2018Document128 pagesDG1 Installation Manual 2018Mario LopezNo ratings yet
- Service Manual Summit HF 03003m July 2017Document105 pagesService Manual Summit HF 03003m July 2017ARMANDOROSAS100% (2)
- №2 Инструкция по эксплуатации двигателя Mitsubishi L2A, L2C, L2B, L3A, L3C, L3E (Operation manual)Document42 pages№2 Инструкция по эксплуатации двигателя Mitsubishi L2A, L2C, L2B, L3A, L3C, L3E (Operation manual)Николай НекрасовNo ratings yet
- Berulit GA 800Document1 pageBerulit GA 800Johan TeoNo ratings yet
- Penton APH30-IP DatasheetDocument2 pagesPenton APH30-IP DatasheetGeorge ZiovasNo ratings yet
- Pump Curve and DefinitionDocument8 pagesPump Curve and DefinitionAleidinNo ratings yet
- A Worn Path SummaryDocument7 pagesA Worn Path SummaryArthas Rhee HermanNo ratings yet
- ForeverDocument3 pagesForeverkathNo ratings yet
- Brief Pain Inventory (Short Form) : Date: Time: NameDocument9 pagesBrief Pain Inventory (Short Form) : Date: Time: NameMarie-Li Dion ParenteauNo ratings yet
- Literatures About PovertyDocument32 pagesLiteratures About PovertyEngel QuimsonNo ratings yet
- DC-8 Tires Fatal Crash Accident Prevention AviationDocument6 pagesDC-8 Tires Fatal Crash Accident Prevention AviationRebecca RiversNo ratings yet
- Missing Chapter SamplerDocument24 pagesMissing Chapter SamplerAllen & UnwinNo ratings yet
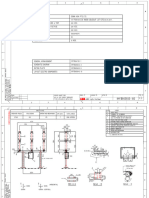
- Drawing CB LTB 145D1 - BDocument9 pagesDrawing CB LTB 145D1 - Btoàn lêNo ratings yet
- Philippine Health Insurance Corporation: Call Center: (02) 8441-7442 Trunkline: (02) 8441-7444Document14 pagesPhilippine Health Insurance Corporation: Call Center: (02) 8441-7442 Trunkline: (02) 8441-7444Jerick Mangiduyos LapurgaNo ratings yet
- Eco FriendlyDocument50 pagesEco FriendlySivakumar K100% (1)