You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Safe Medicate CalculationsDocument4 pagesSafe Medicate Calculationsbe_xx1450% (8)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Cymbalta Case AnalysisDocument9 pagesCymbalta Case AnalysisKeenan SlenkerNo ratings yet
- QA & QC in Clinical TrialDocument54 pagesQA & QC in Clinical Trialpavan_bagga95% (20)
- Investigators BrochureDocument31 pagesInvestigators Brochurepavan_bagga100% (3)
- Yellow Card Spontaneous MonitoringDocument34 pagesYellow Card Spontaneous Monitoringpavan_baggaNo ratings yet
- Declaration End Trial FormDocument2 pagesDeclaration End Trial Formpavan_baggaNo ratings yet
- Belmont Report - 06 Dec10Document17 pagesBelmont Report - 06 Dec10pavan_baggaNo ratings yet
- Comparing Medical Device Law & Reg of Japan, US, and EUDocument5 pagesComparing Medical Device Law & Reg of Japan, US, and EUpavan_baggaNo ratings yet
- Bio Availiility EquivalenceDocument48 pagesBio Availiility Equivalencepavan_baggaNo ratings yet
- Audit of A Clinical Trial SiteDocument30 pagesAudit of A Clinical Trial Sitepavan_baggaNo ratings yet
- ClindamycinDocument1 pageClindamycinTanalie Dulawan75% (4)
- Virlix DrugDocument2 pagesVirlix DrugMsOrangeNo ratings yet
- Pyrosid CapsuleDocument3 pagesPyrosid Capsulehk_scribdNo ratings yet
- BiopharmaceuticsDocument2 pagesBiopharmaceuticsKaela LizadoNo ratings yet
- Adding Medications To Intravenous Fluid ContainersDocument2 pagesAdding Medications To Intravenous Fluid ContainersJemina Rafanan RacadioNo ratings yet
- M. Pharm Review NAPLEX38Document1 pageM. Pharm Review NAPLEX38JUSASBNo ratings yet
- Administering Oral Medication ScriptDocument4 pagesAdministering Oral Medication ScriptJoanna MontebonNo ratings yet
- Drug Schedule Consolidated JEDocument39 pagesDrug Schedule Consolidated JEBryan CoNo ratings yet
- List of PRODUCT SUBMITTED FOR REGISTRATION-ACTIVE INGREDIENT 24-10Document52 pagesList of PRODUCT SUBMITTED FOR REGISTRATION-ACTIVE INGREDIENT 24-10nimirani2012No ratings yet
- 5 - AntiseptikDocument2 pages5 - AntiseptikAlifia Nur RizkiNo ratings yet
- Farmakologi Obat-Obat Yang Bekerja Pada KulitDocument23 pagesFarmakologi Obat-Obat Yang Bekerja Pada KulitReisa Renjisa100% (1)
- Mitomycin - UsmanDocument3 pagesMitomycin - UsmanSittie Nashieva A. UsmanNo ratings yet
- Dissolution MethodsDocument248 pagesDissolution MethodsAnzhela GrigoryanNo ratings yet
- Drug StudyDocument11 pagesDrug StudyLuriel BancasoNo ratings yet
- Format Lplpo 2021Document228 pagesFormat Lplpo 2021Titania PuspaNo ratings yet
- Ch4 Cost-Minimization Analysis PDFDocument12 pagesCh4 Cost-Minimization Analysis PDFAhmad Makhlouf100% (1)
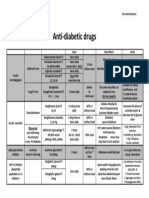
- Anti Diabetic DrugsDocument1 pageAnti Diabetic DrugsWael hadNo ratings yet
- Anesthesia & Muscle Relaxant: Midzocule 10 Bupicule Heavy 0.5%Document3 pagesAnesthesia & Muscle Relaxant: Midzocule 10 Bupicule Heavy 0.5%Shaikh AyyubNo ratings yet
- Tarlac State University College of Science Department of NursingDocument2 pagesTarlac State University College of Science Department of NursingTroy MagcalasNo ratings yet
- LPLPO Puskesmas 2023Document200 pagesLPLPO Puskesmas 2023winn slashNo ratings yet
- Estocott List 2023Document12 pagesEstocott List 2023noorkhaan013No ratings yet
- The Clinical Toxicology of Caffeine: A Review and Case StudyDocument12 pagesThe Clinical Toxicology of Caffeine: A Review and Case Studydita putriNo ratings yet
- Rahul Hospital ReportDocument24 pagesRahul Hospital ReportHritik Chaubey100% (1)
- Laporan Stock OpnameDocument63 pagesLaporan Stock OpnameRian AkäNo ratings yet
- In Biosimilar Guidelines - Feb 17, 2014Document28 pagesIn Biosimilar Guidelines - Feb 17, 2014Aparna ShejwalkarNo ratings yet
- Oktober 2017Document195 pagesOktober 2017Barkah Gitu AjaNo ratings yet
- Anexa CANAMED Fișier Transparență OriginalDocument449 pagesAnexa CANAMED Fișier Transparență Originalcristina ovidenieNo ratings yet
- Respiratory Pharmacology: With Dr. Pravin J. ShukleDocument28 pagesRespiratory Pharmacology: With Dr. Pravin J. ShukleKaish DahiyaNo ratings yet