You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Dental Consent FormDocument2 pagesDental Consent Formkoshimannu100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Emotional Freedom Technics 101Document71 pagesEmotional Freedom Technics 101Nill SalunkeNo ratings yet
- 10 Exogenous Ochronosis in A Chinese Patient Use ofDocument3 pages10 Exogenous Ochronosis in A Chinese Patient Use ofGunawan SamosirNo ratings yet
- Carcinogenesis: Dr. Elisna Syahrudddin, PHD, SP.P (K)Document57 pagesCarcinogenesis: Dr. Elisna Syahrudddin, PHD, SP.P (K)Gunawan SamosirNo ratings yet
- Anatomy RespDocument57 pagesAnatomy RespGunawan SamosirNo ratings yet
- Obat KankerDocument14 pagesObat KankerGunawan SamosirNo ratings yet
- Autonomic Nervous SystemDocument20 pagesAutonomic Nervous SystemGunawan SamosirNo ratings yet
- Ewan Gintings LapkasDocument25 pagesEwan Gintings LapkasGunawan SamosirNo ratings yet
- PosturaldrainageDocument10 pagesPosturaldrainageGunawan SamosirNo ratings yet
- Acute Abdomen For EP: Prasit Wuthisuthimethawee Department of Emergency Medicine Prince of Songkla UniversityDocument77 pagesAcute Abdomen For EP: Prasit Wuthisuthimethawee Department of Emergency Medicine Prince of Songkla UniversityGunawan SamosirNo ratings yet
- Dasar Faal ParuDocument30 pagesDasar Faal ParuGunawan SamosirNo ratings yet
- Medical RecordsMedical ReportsDocument24 pagesMedical RecordsMedical ReportshaasviniNo ratings yet
- OcdDocument9 pagesOcdapi-334485329No ratings yet
- Gastrointestinal Hemorrhage: Carolyn A. Sullivan, MD Pediatric GastroenterologyDocument24 pagesGastrointestinal Hemorrhage: Carolyn A. Sullivan, MD Pediatric GastroenterologyRuntika DewiNo ratings yet
- CXL Te Istanbul 2011Document59 pagesCXL Te Istanbul 2011Ana_BiosooftNo ratings yet
- MCQ Adaptive and Innate Immunity SET-ADocument4 pagesMCQ Adaptive and Innate Immunity SET-AParvathy Sarma100% (1)
- Project Proposal: Barangay Gibraltar Office of The Punong BarangayDocument1 pageProject Proposal: Barangay Gibraltar Office of The Punong BarangayAida Potacag BuasenNo ratings yet
- Medical Nursing I MCQs .Document7 pagesMedical Nursing I MCQs .naa Adel 01No ratings yet
- Polypharmacy in The ElderlyDocument9 pagesPolypharmacy in The ElderlyTugasbu CicikNo ratings yet
- Lumbar Puncture: What You Should KnowDocument5 pagesLumbar Puncture: What You Should KnowQueen SiLogNo ratings yet
- Module 5 Study Guide Postpartum Care19Document2 pagesModule 5 Study Guide Postpartum Care19Lora Ferrer AquinoNo ratings yet
- Automatic Stop OrdersDocument1 pageAutomatic Stop OrdersHartiniNo ratings yet
- R1 Angeles PampangaDocument66 pagesR1 Angeles PampangabalmoresvhienNo ratings yet
- Patient-Centred CareDocument15 pagesPatient-Centred CareMwanja MosesNo ratings yet
- Gonzalez Vs Stonegate Pharmacy 2Document11 pagesGonzalez Vs Stonegate Pharmacy 2Anonymous Pb39klJNo ratings yet
- Mucogingival ConditionsDocument2 pagesMucogingival ConditionsMuhammad Adel100% (1)
- Brain TumorDocument1 pageBrain TumorChase XerolfNo ratings yet
- Hydrogen Peroxide Cancer TreatmentDocument25 pagesHydrogen Peroxide Cancer TreatmentLoreen100% (2)
- Pediatrics Acute AbdomenDocument67 pagesPediatrics Acute AbdomenCabdi IshakNo ratings yet
- Diagnosis Hepatitis PDFDocument18 pagesDiagnosis Hepatitis PDFYuendri IrawantoNo ratings yet
- Hemodialysis: NURSING DIAGNOSIS: Injury, Risk For (Loss of Vascular Access) Risk Factors May IncludeDocument10 pagesHemodialysis: NURSING DIAGNOSIS: Injury, Risk For (Loss of Vascular Access) Risk Factors May IncludeChevelle Valenciano-GaanNo ratings yet
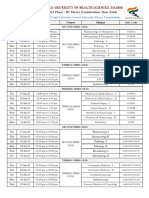
- Summer - 2023 Phase - III Time Table Remaining UG - PG and University Courses University Theory Examinations - 190523Document66 pagesSummer - 2023 Phase - III Time Table Remaining UG - PG and University Courses University Theory Examinations - 190523shivaNo ratings yet
- 20604-Article Text-65316-2-10-20180726 PDFDocument8 pages20604-Article Text-65316-2-10-20180726 PDFMALIK MANASRAHNo ratings yet
- Management of Variceal HemorrhageDocument84 pagesManagement of Variceal HemorrhageFerry SahraNo ratings yet
- Rheumatoid Arthritis: By: Claudio Wangta Oky CahyantoDocument18 pagesRheumatoid Arthritis: By: Claudio Wangta Oky CahyantoEditya AprilianiNo ratings yet
- Case Pres Final ManuscriptDocument30 pagesCase Pres Final ManuscriptSjerwin Anthony GiananNo ratings yet
- Drug Utilisation EvaluationDocument43 pagesDrug Utilisation Evaluationpavani valluriNo ratings yet
- Vaccine Misapplication: Animal SciencesDocument6 pagesVaccine Misapplication: Animal SciencesMohamed AbdelmageedNo ratings yet
- 04 Pediatri Spotleri 2020Document104 pages04 Pediatri Spotleri 2020Osama E. ShamsNo ratings yet