You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- NPK Auto Lube SystemDocument59 pagesNPK Auto Lube SystemLuka Borna100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Class 8 - Maths - Understanding Quadrilaterals PDFDocument32 pagesClass 8 - Maths - Understanding Quadrilaterals PDFAnand MekalaNo ratings yet
- Interlab g26 User's Manual 1.2Document61 pagesInterlab g26 User's Manual 1.2Ali AminiNo ratings yet
- 6-Transport System in Ancient IndiaDocument69 pages6-Transport System in Ancient IndiaAshok Nene100% (1)
- Study The Correlation of Clinker Quality, Reside, PSD On The Performance of Portland CementDocument12 pagesStudy The Correlation of Clinker Quality, Reside, PSD On The Performance of Portland CementIAEME PublicationNo ratings yet
- Assistant Director (Environment) BPS-17Document23 pagesAssistant Director (Environment) BPS-17nomanNo ratings yet
- Weldable Clips - W10: Raillok™ SeriesDocument2 pagesWeldable Clips - W10: Raillok™ SeriesBorislav StoychevNo ratings yet
- Tretinoin (All Trans Retinoic Acid)Document2 pagesTretinoin (All Trans Retinoic Acid)GabrielNo ratings yet
- R GCVP V2 2.15Document3 pagesR GCVP V2 2.15GabrielNo ratings yet
- Pentostatin V4 6.14Document2 pagesPentostatin V4 6.14GabrielNo ratings yet
- R Bendamustine 90 For Low Grade NHL V2 2.15Document2 pagesR Bendamustine 90 For Low Grade NHL V2 2.15GabrielNo ratings yet
- Nilotinib V4 4.13Document2 pagesNilotinib V4 4.13GabrielNo ratings yet
- Melphalan Oral V3 7.11Document2 pagesMelphalan Oral V3 7.11GabrielNo ratings yet
- Intravenous Mel Dex July 08 Checked in Date Oct 2011Document2 pagesIntravenous Mel Dex July 08 Checked in Date Oct 2011GabrielNo ratings yet
- Flag V7 3.15Document2 pagesFlag V7 3.15GabrielNo ratings yet
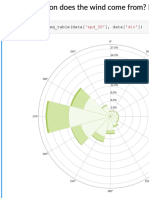
- Predicting The Wind: Data Science in Wind Resource AssessmentDocument61 pagesPredicting The Wind: Data Science in Wind Resource AssessmentFlorian RoscheckNo ratings yet
- Chapter 1 - Introduction To GeologyDocument37 pagesChapter 1 - Introduction To GeologynnsNo ratings yet
- Organic DPPDocument11 pagesOrganic DPPRahul KumarNo ratings yet
- Jan 17 S3Document30 pagesJan 17 S34ydprasadNo ratings yet
- Grade VII ScienceDocument20 pagesGrade VII ScienceSunny BbaNo ratings yet
- Typical 18th Century Sugar EstateDocument9 pagesTypical 18th Century Sugar EstateVernon WhiteNo ratings yet
- Candi Borobudur Dalam Bahasa InggrisDocument5 pagesCandi Borobudur Dalam Bahasa InggrisabdussamadNo ratings yet
- Air Line Filter: Operating Instructions & Parts ManualDocument18 pagesAir Line Filter: Operating Instructions & Parts ManualZeckNo ratings yet
- 966f Interactivo Esquema ElectricDocument8 pages966f Interactivo Esquema ElectricJavierNo ratings yet
- Shigley's Mechanical Engineering DesignDocument39 pagesShigley's Mechanical Engineering Design賴信宏No ratings yet
- Azurian Calidity PDFDocument3 pagesAzurian Calidity PDFfirod63524No ratings yet
- IPP Pahalnar 2 MW DPR FinalDocument279 pagesIPP Pahalnar 2 MW DPR FinalManoj PatneNo ratings yet
- Star Wires India LimitedDocument10 pagesStar Wires India LimitedDesh Deepak0% (1)
- Board Reviewer in PhyChePri - pdf-1Document1 pageBoard Reviewer in PhyChePri - pdf-1Garcia RaphNo ratings yet
- Assignment For Diwali BreakDocument16 pagesAssignment For Diwali BreakArshNo ratings yet
- STD 5 - English - Adjectives Degrees of ComparisonDocument4 pagesSTD 5 - English - Adjectives Degrees of ComparisonReshma KatariaNo ratings yet
- PAS Bhs Inggris XIIDocument5 pagesPAS Bhs Inggris XIIRahmi ZulhidayatiNo ratings yet
- Crystallinity and Transition Temperatures in PolymersDocument46 pagesCrystallinity and Transition Temperatures in PolymersghenisNo ratings yet
- Winsor Pilates - Tips, and Some Exercises To DoDocument8 pagesWinsor Pilates - Tips, and Some Exercises To DoudelmarkNo ratings yet
- HydraGO-brochure WebDocument2 pagesHydraGO-brochure WebRiego GeomembranaNo ratings yet
- Mit Probability Recoitations 3Document3 pagesMit Probability Recoitations 3Kaphun KrubNo ratings yet
- Repair Manual: ZF Getriebe GMBH SaarbrückenDocument200 pagesRepair Manual: ZF Getriebe GMBH Saarbrückenkorol965No ratings yet
- SPRO74 78 94 98 Series JDocument483 pagesSPRO74 78 94 98 Series JRosiane MarcelinoNo ratings yet