You might also like
- Inspection Checklist - Drill RigDocument2 pagesInspection Checklist - Drill RigDuvan Bence83% (30)
- Building (Office) OHS Audit-Assessmnt Form (KF)Document9 pagesBuilding (Office) OHS Audit-Assessmnt Form (KF)bayu arwiansyah100% (2)
- Appendix 15. ALDAR Fire Safety Audit ChecklistDocument10 pagesAppendix 15. ALDAR Fire Safety Audit ChecklistXtreme-DesignsNo ratings yet
- Excavation permit-KSABDocument3 pagesExcavation permit-KSABAdeniran IdrisNo ratings yet
- Form Permit To WorkPermit To WorkDocument1 pageForm Permit To WorkPermit To WorkFaisel Raheem100% (1)
- Sprinkler System ChecklistDocument2 pagesSprinkler System ChecklistJhe Inibam100% (3)
- Bulk Carrier - General Cargo - Container Vessel Survey Report R1.3 FullDocument27 pagesBulk Carrier - General Cargo - Container Vessel Survey Report R1.3 FullKurupath SidharthanNo ratings yet
- Departmental Inspection ChecklistDocument10 pagesDepartmental Inspection Checklistthongtn2007No ratings yet
- RLM 252 MODU 8 06 WDocument5 pagesRLM 252 MODU 8 06 WzaladsNo ratings yet
- Ohs-Pr-09-09-F33 (A) General Hygiene InspectionDocument2 pagesOhs-Pr-09-09-F33 (A) General Hygiene InspectionSiddiquiNo ratings yet
- q1 Template Fire Risk Assessment Simply DocsDocument16 pagesq1 Template Fire Risk Assessment Simply DocsSadkatul BariNo ratings yet
- Security Drill ReportDocument10 pagesSecurity Drill ReporthutsonianpNo ratings yet
- SMM 12 Hot Work PermitDocument4 pagesSMM 12 Hot Work PermitPavan mylapalliNo ratings yet
- Inspection Checklist Drill Rig PDFDocument2 pagesInspection Checklist Drill Rig PDFAbdo Ojaimy100% (2)
- RA 002 - D.O. Tank Inspection and CleaningDocument6 pagesRA 002 - D.O. Tank Inspection and Cleaningdassi99100% (1)
- Annexure I: Block / Building Fire Safety Audit-Check List Fire Safety Audit ChecklistDocument5 pagesAnnexure I: Block / Building Fire Safety Audit-Check List Fire Safety Audit ChecklistGaurav Singh67% (3)
- F 5.3 C Star-Safety-Inspection-ISHTAYAQUEDocument4 pagesF 5.3 C Star-Safety-Inspection-ISHTAYAQUESn AhsanNo ratings yet
- Sample Fire Drill RecordsDocument4 pagesSample Fire Drill RecordsS Bushan100% (2)
- Fire Assessment Audit Checklist October 2023Document5 pagesFire Assessment Audit Checklist October 2023sumasrigkNo ratings yet
- Checklist For Work at Height 13.02.01 HSE OCP-04 F-01 R-1Document1 pageChecklist For Work at Height 13.02.01 HSE OCP-04 F-01 R-1Sabari StunnerNo ratings yet
- Sample Confined Space Entry Permits: Use With Confined Spaces Book, Chapter 296-809 WACDocument7 pagesSample Confined Space Entry Permits: Use With Confined Spaces Book, Chapter 296-809 WACAl Amine Baye FallNo ratings yet
- Risk Management Office Safety Checklist 2014Document2 pagesRisk Management Office Safety Checklist 2014Orxan TalibzadeNo ratings yet
- SWPPP Construction Inspection ReportDocument7 pagesSWPPP Construction Inspection Reportlamintun109.110.111No ratings yet
- Confined Space Checklist Location / Area: Company Name: Date: Requirements Yes No N/ADocument1 pageConfined Space Checklist Location / Area: Company Name: Date: Requirements Yes No N/ASaleem AkhtarNo ratings yet
- HSE-F-NEOM-018 - Weekly Site Safety Inspection ChecklistDocument3 pagesHSE-F-NEOM-018 - Weekly Site Safety Inspection ChecklistAhmed MohamedNo ratings yet
- White Line Formal Safety Risk Assessment Chapter OR 27Document2 pagesWhite Line Formal Safety Risk Assessment Chapter OR 27amirouche15No ratings yet
- Annexure I: Block / Building Fire Safety Audit-Check List Fire Safety Audit ChecklistDocument5 pagesAnnexure I: Block / Building Fire Safety Audit-Check List Fire Safety Audit ChecklistANIL KUMAR M100% (1)
- Boom Concrete Pump ChecklistDocument2 pagesBoom Concrete Pump ChecklistVilky VargheseNo ratings yet
- Confined Space PermitDocument7 pagesConfined Space PermitRamasubramanian SankaranarayananNo ratings yet
- Safety Inspection Check ListDocument24 pagesSafety Inspection Check ListSarah MclaughlinNo ratings yet
- FRM-2530-03 Daily Site Inspection Checkllist Ver - 00Document4 pagesFRM-2530-03 Daily Site Inspection Checkllist Ver - 00Ali KaziNo ratings yet
- Safety Audit Checksheet-1Document8 pagesSafety Audit Checksheet-1Rohit BorudeNo ratings yet
- Checklist For 5-Star Safety Documentation-SOADocument15 pagesChecklist For 5-Star Safety Documentation-SOAYASIRNo ratings yet
- Office Inspection Checklist: Faculty / Other Area (Foa) Information DateDocument4 pagesOffice Inspection Checklist: Faculty / Other Area (Foa) Information Dategeo coach2020No ratings yet
- Laydown Inspection ChecklistDocument1 pageLaydown Inspection ChecklistFahad ChugtaiNo ratings yet
- R 03 Lifting and Shifting Work PermitDocument3 pagesR 03 Lifting and Shifting Work PermitPRIYESH . K. PRIYANNo ratings yet
- Section 3.0.2 Core Drilling Hazard Inspection ListDocument3 pagesSection 3.0.2 Core Drilling Hazard Inspection ListAndi Mangaraja Lubis0% (1)
- L6.21 Blank Office Safety ChecklistDocument3 pagesL6.21 Blank Office Safety ChecklistSubzone ThreeNo ratings yet
- Daily Checklist For SWPDocument2 pagesDaily Checklist For SWPtfpl hseNo ratings yet
- MSD252LGC - Liquefied Gas Carrier Safety Inspection FormDocument3 pagesMSD252LGC - Liquefied Gas Carrier Safety Inspection FormcatalinNo ratings yet
- Pages From Safety Bulletin 2007-1 - Rev 8 Sept 30 2014Document2 pagesPages From Safety Bulletin 2007-1 - Rev 8 Sept 30 2014Mohammed Jahanzeb ChoudaryNo ratings yet
- Ref No: 001/RA/06 Activity Risk Assessment Data Sheet Date: Work Activity: Location Designation: Signature: Date: 25/07/06 Assessment TeamDocument6 pagesRef No: 001/RA/06 Activity Risk Assessment Data Sheet Date: Work Activity: Location Designation: Signature: Date: 25/07/06 Assessment TeamShijad PaNo ratings yet
- A Uh 0417Document17 pagesA Uh 0417Murugan ShanmugaiahNo ratings yet
- Safety Representative Inspection ChecklistDocument5 pagesSafety Representative Inspection ChecklistCandiceNo ratings yet
- CO22 Electric Tools Check ListDocument1 pageCO22 Electric Tools Check ListJansen SungaNo ratings yet
- Enclosed/ Confined Space Entry Permit: As Per ISGOTT - Chapter 10Document4 pagesEnclosed/ Confined Space Entry Permit: As Per ISGOTT - Chapter 10irakli100% (2)
- E & I Audit Sheet Dec11Document5 pagesE & I Audit Sheet Dec11saji kumarNo ratings yet
- LF-D 004A LAPORAN INSPEKSI KAPAL - Vessel Inspection Report (2nd)Document41 pagesLF-D 004A LAPORAN INSPEKSI KAPAL - Vessel Inspection Report (2nd)alsitor100% (1)
- LPS - Short Condition Survey Report Form - MEHRAN EXPLORERDocument4 pagesLPS - Short Condition Survey Report Form - MEHRAN EXPLORERpgupta71No ratings yet
- HSE Inspection Tour ChecklistDocument3 pagesHSE Inspection Tour ChecklistMelchor MolinoNo ratings yet
- NE SHE Monthly Inspection ChecklistDocument3 pagesNE SHE Monthly Inspection ChecklistNarantsatsralt RavdandorjNo ratings yet
- Facility Inspection ChecklistDocument9 pagesFacility Inspection ChecklistdesignselvaNo ratings yet
- Office ChecklistDocument1 pageOffice ChecklistSyed Zakir HassanNo ratings yet
- Code of Safe Working Practices for Merchant Seafarers Consolidated 2015 edition, including amendments 1-7From EverandCode of Safe Working Practices for Merchant Seafarers Consolidated 2015 edition, including amendments 1-7No ratings yet
- Geotechnical Interpretations in Field Practice: An IntroductionFrom EverandGeotechnical Interpretations in Field Practice: An IntroductionNo ratings yet
- Ship's MeasurementDocument7 pagesShip's MeasurementRajeev Rey100% (1)
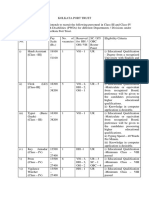
- Kolkata Port PDFDocument2 pagesKolkata Port PDFAnoop Anandan PayyappillyNo ratings yet
- D S SDocument1 pageD S SAnoop Anandan PayyappillyNo ratings yet
- International Legislation: A: International Maritime OrganizationDocument11 pagesInternational Legislation: A: International Maritime OrganizationAnoop Anandan PayyappillyNo ratings yet
- DMLC Certificate Issuing Proc PDFDocument17 pagesDMLC Certificate Issuing Proc PDFAnoop Anandan PayyappillyNo ratings yet
- Marpol Suplement 2015Document48 pagesMarpol Suplement 2015CvitaCvitićNo ratings yet
- Solas 111Document49 pagesSolas 111Anoop Anandan Payyappilly100% (2)
- Handover Check List (Mate) : Ns 092 Issue 1 Rev 2Document2 pagesHandover Check List (Mate) : Ns 092 Issue 1 Rev 2Anoop Anandan PayyappillyNo ratings yet
- Principles of Ship's Stability: Petras PiksrysDocument102 pagesPrinciples of Ship's Stability: Petras Piksryshiginio.moro6182100% (1)
- Evacuation of Passenger Ships PDFDocument30 pagesEvacuation of Passenger Ships PDFAnoop Anandan PayyappillyNo ratings yet
- Northstar Shipping (Aberdeen) Limited Lsa and Medical Planned Maintenance Manual Changes and ModificationsDocument57 pagesNorthstar Shipping (Aberdeen) Limited Lsa and Medical Planned Maintenance Manual Changes and ModificationsAnoop Anandan PayyappillyNo ratings yet
- D S SDocument1 pageD S SAnoop Anandan PayyappillyNo ratings yet
- PSC FSIAnnualReport2012Document62 pagesPSC FSIAnnualReport2012Anoop Anandan PayyappillyNo ratings yet
- Fsi Cir 10Document3 pagesFsi Cir 10Anoop Anandan PayyappillyNo ratings yet
- Nokia TipsDocument7 pagesNokia TipsAnoop Anandan PayyappillyNo ratings yet
- Learn French - Book 2 of 3Document25 pagesLearn French - Book 2 of 3Ber WeydeNo ratings yet
- Learning French EbookDocument36 pagesLearning French EbookDonnette Davis100% (20)
- Learn French - Book 3 of 3Document20 pagesLearn French - Book 3 of 3Ber WeydeNo ratings yet
- Learning Italian EbookDocument27 pagesLearning Italian EbookDonnette Davis100% (16)
- Learn FrenchDocument249 pagesLearn Frenchv155r97% (89)
- LLBDocument1 pageLLBAnoop Anandan PayyappillyNo ratings yet
- 04/06/2011 1 Result of Second Year Supplementary Examination September 2010Document133 pages04/06/2011 1 Result of Second Year Supplementary Examination September 2010Anoop Anandan PayyappillyNo ratings yet
- Omae2005 67123Document8 pagesOmae2005 67123Anoop Anandan PayyappillyNo ratings yet