You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 1047Document1,149 pages1047MANG82% (11)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Enhancing Mitochondrial Function With D RiboseDocument6 pagesEnhancing Mitochondrial Function With D RiboseLeanne Montgomery100% (1)
- Maui's Top Natural RemediesDocument57 pagesMaui's Top Natural RemediesDennisNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- DR - Umpierrere2012 2013 4Document70 pagesDR - Umpierrere2012 2013 4Roberto RamosNo ratings yet
- CRT Test BanksDocument257 pagesCRT Test BanksRain Catan Gagarra Saquin100% (2)
- PACKRAT Cardio Questions PDFDocument63 pagesPACKRAT Cardio Questions PDFkat100% (1)
- Congenital Heart DefectsDocument13 pagesCongenital Heart DefectsGheluzee Herrera100% (2)
- Emergency Exam7Document8 pagesEmergency Exam7Nader Smadi50% (2)
- EntrestoDocument39 pagesEntrestonikhilNo ratings yet
- Cardiovascular System: Guide to the Heart, Blood Vessels, Blood Flow, and Heart FailureDocument43 pagesCardiovascular System: Guide to the Heart, Blood Vessels, Blood Flow, and Heart Failuretruefriends0809No ratings yet
- CHF Case StudyDocument38 pagesCHF Case StudyMelissa David100% (1)
- Soap RoutineDocument3 pagesSoap RoutineRoberto Ramos100% (1)
- Cardiogenic ShockDocument49 pagesCardiogenic Shockmaibejose0% (1)
- Test Bank For Essentials of Pathophysiology 3rd Edition, PorthDocument23 pagesTest Bank For Essentials of Pathophysiology 3rd Edition, PorthILL110100% (1)
- 50 Item Medical-Surgical Nursing Test DrillDocument17 pages50 Item Medical-Surgical Nursing Test DrillFilipino Nurses CentralNo ratings yet
- Clinical CaseDocument10 pagesClinical CaseRoberto RamosNo ratings yet
- Case 3Document8 pagesCase 3Roberto RamosNo ratings yet
- Rhie Full OcrDocument120 pagesRhie Full OcrRoberto RamosNo ratings yet
- Long Case Presentation FINAL-5Document7 pagesLong Case Presentation FINAL-5Roberto RamosNo ratings yet
- Case 4Document8 pagesCase 4Roberto RamosNo ratings yet
- Long Case Presentation FINAL-33Document7 pagesLong Case Presentation FINAL-33Roberto RamosNo ratings yet
- History: Chief Complaint: History of Present Illness: Patient Is A 59 Year Old G6 P1051 Woman Who Is An Inmate That WasDocument9 pagesHistory: Chief Complaint: History of Present Illness: Patient Is A 59 Year Old G6 P1051 Woman Who Is An Inmate That WasRoberto RamosNo ratings yet
- Case 2 AlmostDocument8 pagesCase 2 AlmostRoberto RamosNo ratings yet
- Universidad de Puerto Rico Mail - (No Subject)Document77 pagesUniversidad de Puerto Rico Mail - (No Subject)Roberto RamosNo ratings yet
- Long Case Presentation FINAL-5Document7 pagesLong Case Presentation FINAL-5Roberto RamosNo ratings yet
- McCowan SGA RiskFactors BJOG 2010Document9 pagesMcCowan SGA RiskFactors BJOG 2010Roberto RamosNo ratings yet
- Radio ObGynDocument1 pageRadio ObGynRoberto RamosNo ratings yet
- Paciente 3Document80 pagesPaciente 3Roberto RamosNo ratings yet
- Final - Answers of Ekg QuizDocument46 pagesFinal - Answers of Ekg QuizRoberto RamosNo ratings yet
- Untitled Spreadsheet 2Document4 pagesUntitled Spreadsheet 2Roberto RamosNo ratings yet
- Progress Note Osce - HIV (1) - 2Document1 pageProgress Note Osce - HIV (1) - 2Roberto RamosNo ratings yet
- "Repaso" Shelf OB - GYN 2 2Document9 pages"Repaso" Shelf OB - GYN 2 2Roberto RamosNo ratings yet
- SEPSIS Case 2014 - August-2Document45 pagesSEPSIS Case 2014 - August-2Roberto RamosNo ratings yet
- Universidad Puerto Rico Manual 1415Document161 pagesUniversidad Puerto Rico Manual 1415Roberto RamosNo ratings yet
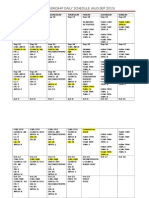
- OB-GYN Clerkship Daily ScheduleDocument3 pagesOB-GYN Clerkship Daily ScheduleRoberto RamosNo ratings yet
- Health Maintenance Cases For Discussion-5Document4 pagesHealth Maintenance Cases For Discussion-5Roberto RamosNo ratings yet
- There Is Been An Overlooked But Important TopicDocument2 pagesThere Is Been An Overlooked But Important TopicRoberto RamosNo ratings yet
- There Is Been An Overlooked But Important TopicDocument2 pagesThere Is Been An Overlooked But Important TopicRoberto RamosNo ratings yet
- HTTPDocument1 pageHTTPRoberto RamosNo ratings yet
- HTTPDocument1 pageHTTPRoberto RamosNo ratings yet
- TAWAKAL Exam BankDocument86 pagesTAWAKAL Exam BankMohamed LibanNo ratings yet
- Lower Limb Edema: Jerin Ann Chelsea Daniel Dinu David Rosin AnnaDocument44 pagesLower Limb Edema: Jerin Ann Chelsea Daniel Dinu David Rosin AnnapalNo ratings yet
- Amniotic Fluid Embolism: Diagnosis and ManagementDocument27 pagesAmniotic Fluid Embolism: Diagnosis and ManagementNino XatiashviliNo ratings yet
- Risk Assessment For Pregnancy With Cardiac Disease-A Global PerspectiveDocument3 pagesRisk Assessment For Pregnancy With Cardiac Disease-A Global PerspectiveAlika MaharaniNo ratings yet
- The Respiratory System: Symptoms, Examination, and SyndromesDocument27 pagesThe Respiratory System: Symptoms, Examination, and SyndromesmiryangelNo ratings yet
- Drug StudyDocument13 pagesDrug Studyapi-3757116100% (4)
- The Impact of Fitness On Surgical Outcomes The.14Document8 pagesThe Impact of Fitness On Surgical Outcomes The.14MIGUEL MORENONo ratings yet
- Diognosa Banding EdemaDocument1 pageDiognosa Banding EdemaMargareth SitorusNo ratings yet
- VHGVHDocument14 pagesVHGVHAlina TashnicNo ratings yet
- Case Study RleDocument25 pagesCase Study Rlelea jumawanNo ratings yet
- Physical Rehabilitation For Older Patients With Acute Decompensated Heart Failure 2021Document19 pagesPhysical Rehabilitation For Older Patients With Acute Decompensated Heart Failure 2021Josemi Del Castillo MolinaNo ratings yet
- HaemoptysisDocument22 pagesHaemoptysisminci sensei100% (5)
- Product Information: Adriamycin Solution For InjectionDocument18 pagesProduct Information: Adriamycin Solution For InjectionArya GuganNo ratings yet
- Wardha PresentationDocument141 pagesWardha PresentationSatyendra OjhaNo ratings yet
- Clinical and Hospital Pharmacy Questionnaire BLUE PACOPDocument39 pagesClinical and Hospital Pharmacy Questionnaire BLUE PACOPSophia AndresNo ratings yet
- Policy Receipt AcknowledgmentDocument35 pagesPolicy Receipt AcknowledgmentKaren de LeonNo ratings yet
- Obstructive Sleep Apnea-Hypopnea SyndromeDocument31 pagesObstructive Sleep Apnea-Hypopnea SyndromeAída TreviñoNo ratings yet