You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- CPA Audit Notes PDFDocument38 pagesCPA Audit Notes PDFMark Butaya100% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- TC1767 Microcontroller Manual PDFDocument1,892 pagesTC1767 Microcontroller Manual PDFpierpaolo aldrigo100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Miyamoto Musashi - The Book of Five RingsDocument34 pagesMiyamoto Musashi - The Book of Five Ringsauto3871No ratings yet
- Differences Between Opinion, Persuasive, and Argument WritingDocument1 pageDifferences Between Opinion, Persuasive, and Argument WritingCláudiaSilvaNo ratings yet
- 11 Crane Frame StructuresDocument6 pages11 Crane Frame StructuresYonas YGNo ratings yet
- Brand Hate Thesis FFFDocument101 pagesBrand Hate Thesis FFFAmbreen ZahraNo ratings yet
- HTML GlossaryDocument6 pagesHTML GlossaryclementNo ratings yet
- 12TH FAIL IntroductionDocument8 pages12TH FAIL Introductiontamilarasijulie4No ratings yet
- Sample Company Presentation PDFDocument25 pagesSample Company Presentation PDFSachin DaharwalNo ratings yet
- Urban Lesson PlanDocument7 pagesUrban Lesson Planapi-265908930No ratings yet
- French RevolutionDocument10 pagesFrench Revolutionwhat I learned in high school100% (26)
- Severe Acute Malnutrition and Fluid Management inDocument76 pagesSevere Acute Malnutrition and Fluid Management inBibsNo ratings yet
- Grade 8 LP (3RD Quarter-4health)Document6 pagesGrade 8 LP (3RD Quarter-4health)Shamaica SurigaoNo ratings yet
- Agg Lika 2006Document3 pagesAgg Lika 2006Georgia GiampoylakiNo ratings yet
- ERICK ALCANTARA MAGDAONG - ResumeDocument2 pagesERICK ALCANTARA MAGDAONG - Resumecathy villanuevaNo ratings yet
- 1 To 12 Calndar 2023-24 Sunita MamDocument17 pages1 To 12 Calndar 2023-24 Sunita MamPoonm ChoudharyNo ratings yet
- An Automated Method For Computer Vision Analysis of Cannon-Launched Artillery VideoDocument12 pagesAn Automated Method For Computer Vision Analysis of Cannon-Launched Artillery VideoyararaNo ratings yet
- Abhishek BTP2xDocument57 pagesAbhishek BTP2xAbhishek SaxenaNo ratings yet
- Dylan Thomas WorksheetDocument2 pagesDylan Thomas WorksheetBelano82No ratings yet
- Exercise - Melting ExpandDocument3 pagesExercise - Melting Expandatik_kurniasihNo ratings yet
- Chapter 6 BWDDocument63 pagesChapter 6 BWDcpawan_699508No ratings yet
- NCP FormatDocument1 pageNCP FormatNathaniel NograNo ratings yet
- Behavioral Finance-Group 14Document6 pagesBehavioral Finance-Group 14Priyanka PawarNo ratings yet
- The Land of Pakistan MCQs For All Type of Competitive ExaminationsDocument10 pagesThe Land of Pakistan MCQs For All Type of Competitive ExaminationsSadia manzoorNo ratings yet
- Long Vowels & Soft Sound-C, G Trigraphs & Imp Sound UnitsDocument4 pagesLong Vowels & Soft Sound-C, G Trigraphs & Imp Sound UnitsNagmaNo ratings yet
- Kinetics 2Document8 pagesKinetics 2likpataNo ratings yet
- Soal T.O Farid IiDocument4 pagesSoal T.O Farid IiPatriot Muda TulungagungNo ratings yet
- Why Stories Are Important: Why Read With Children? How Books and Stories Help ChildrenDocument4 pagesWhy Stories Are Important: Why Read With Children? How Books and Stories Help ChildrenChristina KiuNo ratings yet
- Eat2Eat V4Document38 pagesEat2Eat V4Manish RYNo ratings yet
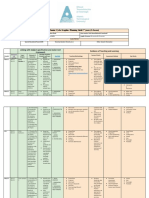
- Planning Grid Junior Cert Graphics 2nd YearsDocument5 pagesPlanning Grid Junior Cert Graphics 2nd Yearsapi-547735446No ratings yet