You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The PhiladelphiaDocument6 pagesThe PhiladelphiaRyan CaddiganNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Flying Star WikiDocument14 pagesFlying Star WikiOwlbear100% (1)
- The Dystopian NovelDocument17 pagesThe Dystopian NovelafiNo ratings yet
- Tension PneumothoraxDocument5 pagesTension PneumothoraxKay BristolNo ratings yet
- Pancha Pakshi Report For CrowDocument16 pagesPancha Pakshi Report For CrowPrasanna BabuNo ratings yet
- Daniel A. Lichtenstein - Lung UsDocument29 pagesDaniel A. Lichtenstein - Lung UsEricka Powers100% (1)
- SDOFM Viscerosomatic Reflex Pocket ChartDocument2 pagesSDOFM Viscerosomatic Reflex Pocket ChartRohit NalamasuNo ratings yet
- Case Study About Cervical CancerDocument11 pagesCase Study About Cervical CancerJisel-Apple Bulan100% (1)
- Guide:-Prof. Dr. V. P. Joglekar Dept. of Agadatantra, Tilak Ayu. Mahavidyalaya, Pune Author: - Dr. Nishant B. BarapatreDocument24 pagesGuide:-Prof. Dr. V. P. Joglekar Dept. of Agadatantra, Tilak Ayu. Mahavidyalaya, Pune Author: - Dr. Nishant B. BarapatreDrNishant Barapatre100% (1)
- Mycobacterium Leprae: DR Retno Budiarti Microbiology DepartmentDocument25 pagesMycobacterium Leprae: DR Retno Budiarti Microbiology DepartmentPrincess QumanNo ratings yet
- IndianJPharmacol493229-3498174 094301Document7 pagesIndianJPharmacol493229-3498174 094301Prasanna BabuNo ratings yet
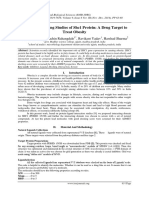
- Molecular Docking Studies of Shc1 Protein: A Drug Target To Treat ObesityDocument6 pagesMolecular Docking Studies of Shc1 Protein: A Drug Target To Treat ObesityPrasanna BabuNo ratings yet
- Detal PasteDocument8 pagesDetal PastePrasanna BabuNo ratings yet
- Fetal Pharmacotherapy PDFDocument17 pagesFetal Pharmacotherapy PDFPrasanna BabuNo ratings yet
- Current Advances in Transdermal Delivery of Drugs For Alzheimer's DiseaseDocument10 pagesCurrent Advances in Transdermal Delivery of Drugs For Alzheimer's DiseasePrasanna BabuNo ratings yet
- Research Paper: Indian J Pharmacol April 2005 Vol 37 Issue 2 103-110Document8 pagesResearch Paper: Indian J Pharmacol April 2005 Vol 37 Issue 2 103-110Prasanna BabuNo ratings yet
- S. K.Ray, S.C. Basak, C.Roychaudhury. A.B.Roy Andj.J. GhoshDocument12 pagesS. K.Ray, S.C. Basak, C.Roychaudhury. A.B.Roy Andj.J. GhoshPrasanna BabuNo ratings yet
- Vol4 Issue6 08Document8 pagesVol4 Issue6 08Prasanna BabuNo ratings yet
- TempDocument2 pagesTempPrasanna BabuNo ratings yet
- Reflections On The Evolution of Pharmacology in India During Twentieth CenturyDocument13 pagesReflections On The Evolution of Pharmacology in India During Twentieth CenturyPrasanna BabuNo ratings yet
- Current Global Status & Impact of Human Papillomavirus Vaccination: Implications For IndiaDocument12 pagesCurrent Global Status & Impact of Human Papillomavirus Vaccination: Implications For IndiaPrasanna BabuNo ratings yet
- IndianJMedRes1442151-3069351 083133Document3 pagesIndianJMedRes1442151-3069351 083133Prasanna BabuNo ratings yet
- File779 4Document76 pagesFile779 4Prasanna BabuNo ratings yet
- File779 4Document76 pagesFile779 4Prasanna BabuNo ratings yet
- Listening Comprehension The Amish ParadiseDocument5 pagesListening Comprehension The Amish ParadiseAngel Angeleri-priftis.100% (2)
- Gastro Lab ManualDocument28 pagesGastro Lab ManualYeniNo ratings yet
- Equine Physical Exam Guide: Common Mistakes When Monitoring Vital SignsDocument1 pageEquine Physical Exam Guide: Common Mistakes When Monitoring Vital Signsvetthamil100% (1)
- Thesis Statement For Animal ResearchDocument5 pagesThesis Statement For Animal Researchtit0feveh1h3100% (1)
- Polar Bear (Report Text)Document14 pagesPolar Bear (Report Text)Adeb Wahyu100% (1)
- Cheat Sheet 2Document2 pagesCheat Sheet 2oushaNo ratings yet
- Spelling of Plural Nouns in English PDFDocument3 pagesSpelling of Plural Nouns in English PDFSamuel PagottoNo ratings yet
- Baylissascaris LarvisDocument136 pagesBaylissascaris LarvisAlejoDubertiNo ratings yet
- Manual de Endodoncia Basica V6Document6 pagesManual de Endodoncia Basica V6evripidis tziokasNo ratings yet
- Sains t2 PDFDocument6 pagesSains t2 PDFSJK CHUNG HUA 4 1/2 四哩半中公No ratings yet
- Formation of Faeces and DefecationDocument11 pagesFormation of Faeces and Defecationbiologi88No ratings yet
- NCERT Class VIII Science Chapter 8 Cell - The Basic Unit of LifeDocument11 pagesNCERT Class VIII Science Chapter 8 Cell - The Basic Unit of LifeAbhasNo ratings yet
- UH Kelas XIIDocument7 pagesUH Kelas XIIElismawati AzmarNo ratings yet
- Case 1Document6 pagesCase 1Nico AguilaNo ratings yet
- Pulmo Physio-Transport 2Document35 pagesPulmo Physio-Transport 2Mich Therese AbejeroNo ratings yet
- Answer Keys of Comedk Pget-2008Document23 pagesAnswer Keys of Comedk Pget-2008mobiled2No ratings yet
- 0610 s17 QP 31Document24 pages0610 s17 QP 31BioScMentor-1No ratings yet
- Pet Insurance: Because Pets Are Family TooDocument10 pagesPet Insurance: Because Pets Are Family ToomeeraNo ratings yet
- Diaphragmatic Breathing: The Foundation of Core StabilityDocument7 pagesDiaphragmatic Breathing: The Foundation of Core StabilityLevyNo ratings yet
- Protochordata FIXDocument33 pagesProtochordata FIXSylvia AnggraeniNo ratings yet
- Gibberish WordsDocument4 pagesGibberish WordsDaniel PopaNo ratings yet