You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Ebook First Aid For The Psychiatry Clerkship Sixth Edition PDF Full Chapter PDFDocument59 pagesEbook First Aid For The Psychiatry Clerkship Sixth Edition PDF Full Chapter PDFgwendolyn.jordan283100% (30)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- ITLS 9e Basic Pre-Test - Version 9.2 - Answer KeysDocument10 pagesITLS 9e Basic Pre-Test - Version 9.2 - Answer KeysNeil ThomasNo ratings yet
- 1.15 IMO Model Course Medical PDFDocument12 pages1.15 IMO Model Course Medical PDFdarrelsilvaNo ratings yet
- Diabetes Medication ChartDocument21 pagesDiabetes Medication CharttmleNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Blood Pressure Medication ChartDocument1 pageBlood Pressure Medication CharttmleNo ratings yet
- Emergency Use Authorization (EUA) For An Unapproved Product Review Memorandum Identifying InformationDocument57 pagesEmergency Use Authorization (EUA) For An Unapproved Product Review Memorandum Identifying InformationNicoleta Eugenia BursucNo ratings yet
- Performance Review NPDocument11 pagesPerformance Review NPtmleNo ratings yet
- Common Illnesses in Family PracticeDocument234 pagesCommon Illnesses in Family Practicetmle100% (2)
- Dental MneumonicDocument30 pagesDental Mneumonictmle44% (9)
- Microbiology and Parasitology - Activity 4 The Control of DiseaseDocument3 pagesMicrobiology and Parasitology - Activity 4 The Control of DiseaseClaro M. GarchitorenaNo ratings yet
- MR-SIA 2023 Annex-E.-Quick-Health-Assessment-FormDocument1 pageMR-SIA 2023 Annex-E.-Quick-Health-Assessment-FormDatu Hoffer RhuNo ratings yet
- Clinical Visit SummaryDocument8 pagesClinical Visit SummaryDemonfoxNo ratings yet
- Mucinosis Por Un FarmadoDocument4 pagesMucinosis Por Un FarmadoLuluu CortésNo ratings yet
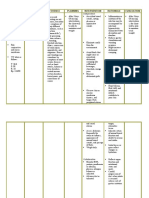
- Nursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument3 pagesNursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationAbdallah AlasalNo ratings yet
- CUC Breast Cancer History and Examination DR Corinne Jones Mar10Document1 pageCUC Breast Cancer History and Examination DR Corinne Jones Mar10starblue265No ratings yet
- Applicant's Information SheetDocument1 pageApplicant's Information Sheetbamstershell 09No ratings yet
- Caring For The ElderlyDocument3 pagesCaring For The Elderlyreinildis malaNo ratings yet
- National HIV Testing and Treatment Guidelines 2020 (Updated) - NepalHealthMagazineDocument156 pagesNational HIV Testing and Treatment Guidelines 2020 (Updated) - NepalHealthMagazineKulgaurav RegmiNo ratings yet
- EyeDocument3 pagesEyeRamon TayagNo ratings yet
- 2022 Clinthera S1T2 Hypercholesterolemia PDFDocument7 pages2022 Clinthera S1T2 Hypercholesterolemia PDFmedicoNo ratings yet
- Pedal EdemaDocument45 pagesPedal Edemafirdaushassan2112No ratings yet
- Diseases of Conjunctiva: 12/08/21 DR Sanjay Shrivastava 1Document118 pagesDiseases of Conjunctiva: 12/08/21 DR Sanjay Shrivastava 1chiryarashdi0% (1)
- Drug StudyDocument2 pagesDrug Studyunkown userNo ratings yet
- The Study of Clinico-Aetiological Profile of Pancytopenia in Elderly PDFDocument3 pagesThe Study of Clinico-Aetiological Profile of Pancytopenia in Elderly PDFKaye Antonette AntioquiaNo ratings yet
- Breathing ExercisesDocument35 pagesBreathing ExercisesShubham KathareNo ratings yet
- INFECTION CONTROL by Sandra WilsonDocument24 pagesINFECTION CONTROL by Sandra WilsonsandraNo ratings yet
- Antibiotic PolicyDocument4 pagesAntibiotic PolicyAchmad Faiz SulaimanNo ratings yet
- Myths Vs Facts About Breast CancerDocument1 pageMyths Vs Facts About Breast CancerNyanaNo ratings yet
- Feline Pyometra PDFDocument2 pagesFeline Pyometra PDFMelvinNo ratings yet
- Obstructive Sleep Apnoea: S.PavithraDocument20 pagesObstructive Sleep Apnoea: S.PavithraSyed Mujtaba Hussain RazviNo ratings yet
- Radiology MCQSDocument23 pagesRadiology MCQSHabib Mughal67% (3)
- Organophosphorus Insecticide Induced Hemorrhagic Pancreatitis - A Case ReportDocument3 pagesOrganophosphorus Insecticide Induced Hemorrhagic Pancreatitis - A Case ReportIOSRjournalNo ratings yet
- Surgical Aphorisms and SayingsDocument5 pagesSurgical Aphorisms and SayingsShriyans Jain100% (1)
- Tuberculosis PPT RDocument29 pagesTuberculosis PPT RRamandeep KaurNo ratings yet
- CES6 - Infectious Disease BookDocument138 pagesCES6 - Infectious Disease Bookarnaldops333No ratings yet