You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Army of Darkness RPG (Core Book) PDFDocument242 pagesArmy of Darkness RPG (Core Book) PDFRukia Sereitei100% (2)
- Earthbag Building in The Humid Tropics, 2nd Ed.Document30 pagesEarthbag Building in The Humid Tropics, 2nd Ed.Patti Stouter100% (4)
- Crye Precision Product Guide 2015Document74 pagesCrye Precision Product Guide 2015Axiom5100% (2)
- Cultivation of Pleurotus Ostreatus and Other Edible MushroomsDocument17 pagesCultivation of Pleurotus Ostreatus and Other Edible MushroomssiripornhassarangseeNo ratings yet
- ENWZGOOBEDocument19 pagesENWZGOOBERukia SereiteiNo ratings yet
- IntroductionToArcMap PDFDocument40 pagesIntroductionToArcMap PDFAlina ManduNo ratings yet
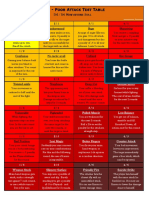
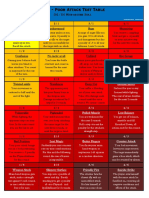
- Earthdawn - Poor Attack Test Table: D4 / D6 Misfortune RollDocument1 pageEarthdawn - Poor Attack Test Table: D4 / D6 Misfortune RollRukia SereiteiNo ratings yet
- Personenindex BarDocument12 pagesPersonenindex BarRukia SereiteiNo ratings yet
- Fern Spore Bank at PedregulhoDocument9 pagesFern Spore Bank at PedregulhoRukia SereiteiNo ratings yet
- Patt v3 (Hard)Document1 pagePatt v3 (Hard)Rukia SereiteiNo ratings yet
- Patt v1 (Easy)Document1 pagePatt v1 (Easy)Rukia SereiteiNo ratings yet
- SR4 101scenariosDocument11 pagesSR4 101scenariosShawn WillettNo ratings yet
- ED U M Editable Char Sheet d12Document3 pagesED U M Editable Char Sheet d12Rukia SereiteiNo ratings yet
- Olfactory Information Saves Venom During Prey-Capture of The Hunting SpiderDocument7 pagesOlfactory Information Saves Venom During Prey-Capture of The Hunting SpiderRukia SereiteiNo ratings yet
- Powerful GroupsDocument8 pagesPowerful GroupsRukia SereiteiNo ratings yet
- The Evolution and Development of Arthropod AppendagesDocument24 pagesThe Evolution and Development of Arthropod AppendagesRukia SereiteiNo ratings yet
- Edara A Steampunk Renaissance Character Sheet (6620904)Document2 pagesEdara A Steampunk Renaissance Character Sheet (6620904)Rukia SereiteiNo ratings yet
- Infidelity - It May Be in Our Genes. Our Cheating HeartsDocument9 pagesInfidelity - It May Be in Our Genes. Our Cheating HeartsRukia SereiteiNo ratings yet
- Terrestrial Snails Aff Ecting Plants in FloridaDocument12 pagesTerrestrial Snails Aff Ecting Plants in FloridaRukia SereiteiNo ratings yet
- Science:, 1205 (2013) John L. HooglandDocument4 pagesScience:, 1205 (2013) John L. HooglandRukia SereiteiNo ratings yet
- Season 5 ContactsDocument12 pagesSeason 5 ContactsRukia SereiteiNo ratings yet
- Building An Earthbag Dome - Rob WainwrightDocument5 pagesBuilding An Earthbag Dome - Rob Wainwrightmanish0210100% (1)