You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- IKEA Business PlanDocument7 pagesIKEA Business PlanOmar SalehNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- AnatomediaDocument4 pagesAnatomediaAli AlamsyahNo ratings yet
- Chapter 6 Unit Test TrigDocument6 pagesChapter 6 Unit Test TrigAnanya Sharma - Lincoln Alexander SS (2132)No ratings yet
- The A To Z of The Coptic ChurchDocument357 pagesThe A To Z of The Coptic ChurchNoso100% (1)
- CT Examination Of: Common IndicationsDocument1 pageCT Examination Of: Common IndicationsAli AlamsyahNo ratings yet
- Patient Preparations: Xial Mages OF THE ArynxDocument1 pagePatient Preparations: Xial Mages OF THE ArynxAli AlamsyahNo ratings yet
- CT Studies O: Neck Mandatory Elective Larynx 3 Soft Tissue 5 Carotid Angiography 3Document1 pageCT Studies O: Neck Mandatory Elective Larynx 3 Soft Tissue 5 Carotid Angiography 3Ali AlamsyahNo ratings yet
- Jumlah Produk Biaya Tetap Biaya Total Biaya Variabel Total Penjualan Biaya Variabel Per Unit Harga Jual Per Unit Biaya Variabel Dibanding PenjualanDocument17 pagesJumlah Produk Biaya Tetap Biaya Total Biaya Variabel Total Penjualan Biaya Variabel Per Unit Harga Jual Per Unit Biaya Variabel Dibanding PenjualanAli AlamsyahNo ratings yet
- Marriageofheaven00blak PDFDocument58 pagesMarriageofheaven00blak PDFMihaela NițăNo ratings yet
- Pol Part in Europe PDFDocument22 pagesPol Part in Europe PDFSheena PagoNo ratings yet
- Framing Effects of Information On Investment Risk PerceptionDocument16 pagesFraming Effects of Information On Investment Risk PerceptionConstanza Caceres VidalNo ratings yet
- Supporting Information Emergency MedicineDocument3 pagesSupporting Information Emergency MedicineHaider Ahmad KamilNo ratings yet
- Official History of Improved Order of RedmenDocument672 pagesOfficial History of Improved Order of RedmenGiniti Harcum El BeyNo ratings yet
- Acceeration MechanismDocument33 pagesAcceeration MechanismDavid nelsonNo ratings yet
- Collected Works of K - A - Krishnaswamy Iyer-2006 PDFDocument341 pagesCollected Works of K - A - Krishnaswamy Iyer-2006 PDFdeepak.marurNo ratings yet
- Read Aloud HoorayDocument4 pagesRead Aloud Hoorayapi-298364857No ratings yet
- 3.1 Thermal PhysicsDocument10 pages3.1 Thermal Physicsmardel11No ratings yet
- All India Final Year Engineering 2023 24 Batch SAMPLE 3Document14 pagesAll India Final Year Engineering 2023 24 Batch SAMPLE 3Since16100% (1)
- FAQs in C LanguageDocument256 pagesFAQs in C LanguageShrinivas A B0% (2)
- M0003 NHLDocument497 pagesM0003 NHLUday kumarNo ratings yet
- Stanislavakian Acting As PhenomenologyDocument21 pagesStanislavakian Acting As Phenomenologybenshenhar768250% (2)
- Final Jury Instructions Seditious Conspiracy Oath KeepersDocument51 pagesFinal Jury Instructions Seditious Conspiracy Oath KeepersDaily KosNo ratings yet
- The Five Commandments of Infectious Disease ControlDocument2 pagesThe Five Commandments of Infectious Disease ControlCarol ReedNo ratings yet
- Posh SQ L Wall ChartDocument1 pagePosh SQ L Wall Chartjoselara19No ratings yet
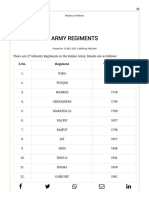
- Army Regiments: S.No. Regiment Year of RaisingDocument3 pagesArmy Regiments: S.No. Regiment Year of RaisingAsc47No ratings yet
- Assignment 3 English Unit PlanDocument8 pagesAssignment 3 English Unit Planapi-626567329No ratings yet
- Britni Freiboth's Resume 2010Document2 pagesBritni Freiboth's Resume 2010api-51238443No ratings yet
- Pay It ForwardDocument5 pagesPay It ForwardCed HernandezNo ratings yet
- Storytelling Is The Conveying of Events in Words, Images, andDocument9 pagesStorytelling Is The Conveying of Events in Words, Images, andly_meyhNo ratings yet
- Dvar Torah FinalDocument5 pagesDvar Torah FinalKarry TaylorNo ratings yet
- Week 8 ActivityDocument4 pagesWeek 8 ActivityEmmanuel SindolNo ratings yet
- Personality Types by Eric PartakerDocument1 pagePersonality Types by Eric Partakermanishmangal2008No ratings yet
- Grade 10 ICT LessonsPlanDocument19 pagesGrade 10 ICT LessonsPlanzarookNo ratings yet
- 2021-09-Network Design and Troubleshooting Assign-PART1Document10 pages2021-09-Network Design and Troubleshooting Assign-PART1Firdous JamalNo ratings yet
- A Report On: Bachelor of Technology IN Civil EngineeringDocument31 pagesA Report On: Bachelor of Technology IN Civil EngineeringKalyan Reddy AnuguNo ratings yet