You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Principles of Healthcare Reimbursement: Sixth EditionDocument28 pagesPrinciples of Healthcare Reimbursement: Sixth EditionDestiny Hayes100% (2)
- Organization ChartDocument1 pageOrganization Chartpankajbhatt376No ratings yet
- Ron Brookmeyer, Donna F. Stroup-Monitoring The Health of Populations - Statistical Principles and Methods For Public Health Surveillance (2003)Document389 pagesRon Brookmeyer, Donna F. Stroup-Monitoring The Health of Populations - Statistical Principles and Methods For Public Health Surveillance (2003)Medical_Doctor100% (1)
- WHODocument22 pagesWHOAshok100% (1)
- Quality Operating Process: Manual of Operations Care of PatientsDocument4 pagesQuality Operating Process: Manual of Operations Care of PatientsPrabhat KumarNo ratings yet
- Review OF Rmnch+A, RCH Including Other Maternal Health Programme and IdspDocument73 pagesReview OF Rmnch+A, RCH Including Other Maternal Health Programme and IdspGargi pandeyNo ratings yet
- Nadra Resume Formatted 082609Document8 pagesNadra Resume Formatted 082609amsalaliNo ratings yet
- Midterm Ca1 (1) CHNDocument7 pagesMidterm Ca1 (1) CHNRheeanne Mae AmilasanNo ratings yet
- Athenahealth: Possible ERP System Modules and Its Features or CharacteristicsDocument3 pagesAthenahealth: Possible ERP System Modules and Its Features or CharacteristicsMaica Joules MontehermosoNo ratings yet
- Pajor, Camille: SubscriberDocument3 pagesPajor, Camille: SubscriberRose LoBue FoleyNo ratings yet
- O'neill Media Release Senate Inquiry Probes Impact of Health Cuts On SydneysidersDocument2 pagesO'neill Media Release Senate Inquiry Probes Impact of Health Cuts On SydneysidersannecharltonNo ratings yet
- Opsdog - KPI-Encyclopedi Healthcare-Management Preview 5pgsDocument5 pagesOpsdog - KPI-Encyclopedi Healthcare-Management Preview 5pgsJohn CheekanalNo ratings yet
- Kpi Aa Ip 2023Document10 pagesKpi Aa Ip 2023Poppy FitraNo ratings yet
- Important News About Your Health Benefits: Jason Schmit 4 Snowapple Irvine, CA 92614Document3 pagesImportant News About Your Health Benefits: Jason Schmit 4 Snowapple Irvine, CA 92614JRSNo ratings yet
- Notice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsDocument1 pageNotice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsJustia.comNo ratings yet
- MDR 010265652269Document1 pageMDR 010265652269Joshua RadocNo ratings yet
- Daftar Buku K3Document5 pagesDaftar Buku K3MaulanaNo ratings yet
- Roger Goodell Memo To TeamsDocument2 pagesRoger Goodell Memo To TeamsHouston ChronicleNo ratings yet
- Management Across The Continuum of Care: Case Management Guide To Population HealthDocument29 pagesManagement Across The Continuum of Care: Case Management Guide To Population Healthkritis ardiansyahNo ratings yet
- A Guide To Methodology in Ergonomics Designing For Human UseDocument10 pagesA Guide To Methodology in Ergonomics Designing For Human UseNew GigameNo ratings yet
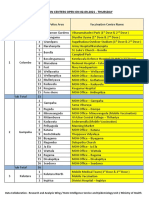
- Vaccination Centers On 02.09.2021Document12 pagesVaccination Centers On 02.09.2021Chanu On CT100% (1)
- Swedish Medical Center Earns 2021 Leapfrog Top Hospital Award For Outstanding Quality and SafetyDocument4 pagesSwedish Medical Center Earns 2021 Leapfrog Top Hospital Award For Outstanding Quality and SafetyPR.comNo ratings yet
- Documentation and Nurse Practitioner RoleDocument5 pagesDocumentation and Nurse Practitioner RoleEnerolisa ParedesNo ratings yet
- Dear ColleagueDocument3 pagesDear ColleaguePeter SullivanNo ratings yet
- 11 Key Areas of ResponsibilityDocument1 page11 Key Areas of ResponsibilitymesdejenNo ratings yet
- Rural Health Midwives Placement Program (RHMPP) / Midwifery Scholarship Program of The Philippines (MSPP)Document5 pagesRural Health Midwives Placement Program (RHMPP) / Midwifery Scholarship Program of The Philippines (MSPP)daryl ann dep-as100% (1)
- OHS-Occupational Safety and Healt TestDocument4 pagesOHS-Occupational Safety and Healt TestHisburn BermudezNo ratings yet
- Epidemiology of Typhoid Fever in The PhilippinesDocument5 pagesEpidemiology of Typhoid Fever in The Philippinesjessica_nava_8No ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore KarnatakaDocument18 pagesRajiv Gandhi University of Health Sciences Bangalore Karnatakapallavi sharmaNo ratings yet
- QSEN and CompetenciesDocument3 pagesQSEN and CompetenciesRegarde Le Ciel IciNo ratings yet