You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- General AnnuitiesDocument141 pagesGeneral AnnuitiesJuanito71% (7)
- Mcs Meaning and ObjectivesDocument6 pagesMcs Meaning and ObjectivesRatheesh KumarNo ratings yet
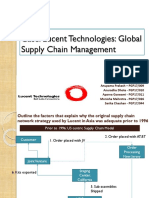
- Lucent Technologies CaseDocument9 pagesLucent Technologies CaseShrivathsan KSNo ratings yet
- Underdevelopment in Africa Theories and FactsDocument15 pagesUnderdevelopment in Africa Theories and FactsFanose GudisaNo ratings yet
- Economic Dev't, PDP SummaryDocument11 pagesEconomic Dev't, PDP SummaryJanell AgananNo ratings yet
- R3S PPT in CWTS DefenseDocument17 pagesR3S PPT in CWTS DefenseErika Mae SanchezNo ratings yet
- Zero Bound Elsarticle-RevisedDocument43 pagesZero Bound Elsarticle-RevisedBrunéNo ratings yet
- Actividad 10 Evidencia 6 Steps To ExportDocument5 pagesActividad 10 Evidencia 6 Steps To ExportRicardo Andres Barrios Vargas100% (3)
- Ebtke Conex 2012 ProposalDocument15 pagesEbtke Conex 2012 ProposalFahmi Adha NurdinNo ratings yet
- Updated HB2279PN3277 063010 9amDocument39 pagesUpdated HB2279PN3277 063010 9amjmicekNo ratings yet
- For425 Lec 1Document29 pagesFor425 Lec 1Sam CherniakNo ratings yet
- Operation ManagementDocument16 pagesOperation ManagementTeoh Rou PeiNo ratings yet
- Atul Kohli - State-Directed Development - Political Power and Industrialization in The Global Periphery (2004)Document480 pagesAtul Kohli - State-Directed Development - Political Power and Industrialization in The Global Periphery (2004)Jeyapragash RNo ratings yet
- Mang Inasal BackgroundDocument2 pagesMang Inasal BackgroundDianne BotecarioNo ratings yet
- Mini Grids Ehs ChecklistDocument3 pagesMini Grids Ehs ChecklistRaina Jessamine GangNo ratings yet
- BOOK WITH BOB'S BAKERY CASE Microeconomics in Context PDFDocument206 pagesBOOK WITH BOB'S BAKERY CASE Microeconomics in Context PDFMwenda MongweNo ratings yet
- Repeal The Casino Deal Sept 5 FilingDocument31 pagesRepeal The Casino Deal Sept 5 FilingMassLiveNo ratings yet
- Challenges in Agribusiness in NigeriaDocument3 pagesChallenges in Agribusiness in NigeriaTomilola Odejayi Balogun50% (2)
- National Income AccountingDocument42 pagesNational Income Accountingraemu26No ratings yet
- 2021 National Budget Highlights ZimbabweDocument14 pages2021 National Budget Highlights ZimbabwenyashaNo ratings yet
- Suriname Food Security Policy and InitiativesDocument11 pagesSuriname Food Security Policy and InitiativesJamal BakarNo ratings yet
- What Is EthicsDocument16 pagesWhat Is EthicsAnsh PreetNo ratings yet
- SJVN Limited: (A Joint Venture of Govt. of India & Govt. of Himachal Pradesh)Document6 pagesSJVN Limited: (A Joint Venture of Govt. of India & Govt. of Himachal Pradesh)SJNo ratings yet
- Chapter 16 QuizDocument3 pagesChapter 16 Quizbeckkl05No ratings yet
- Sadia Saeed EconomicsDocument15 pagesSadia Saeed Economicssadia saeedNo ratings yet
- Process Mapping at Raymond Ltd.Document6 pagesProcess Mapping at Raymond Ltd.Aditi Yadav100% (1)
- Chapter 1: Nature and Scope of Economics: Unit 1: IntroductionDocument2 pagesChapter 1: Nature and Scope of Economics: Unit 1: Introductionvasantha mulpuriNo ratings yet
- Manifest Lapak CBR & Lapak Ciliwung AprilDocument48 pagesManifest Lapak CBR & Lapak Ciliwung AprilLapack CiliwungNo ratings yet
- Lcasean Midterms Part 1Document5 pagesLcasean Midterms Part 1Sid Damien TanNo ratings yet