You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- CVS Essay QuestionsDocument3 pagesCVS Essay QuestionsPeter AbikoyeNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ancel Keys StudyDocument17 pagesAncel Keys Studyapi-310369776No ratings yet
- Bateman Fonagy 2008 Mentalization Based Treatment For BPDDocument16 pagesBateman Fonagy 2008 Mentalization Based Treatment For BPDCamila Piña SanhuezaNo ratings yet
- Dental MneumonicDocument30 pagesDental Mneumonictmle44% (9)
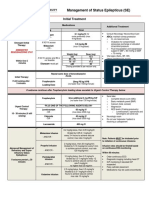
- Status EpilepticusDocument6 pagesStatus Epilepticussandykumala100% (1)
- PsychopharmacologyDocument53 pagesPsychopharmacologypujarze4100% (1)
- Term PaperDocument4 pagesTerm PaperIvin KuriakoseNo ratings yet
- CA EsophagusDocument37 pagesCA EsophagusElandha PutriNo ratings yet
- What Is RH IncompatibilityDocument22 pagesWhat Is RH IncompatibilityKimsha ConcepcionNo ratings yet
- Dizziness: Classification and PathophysiologyDocument16 pagesDizziness: Classification and Pathophysiologyrapannika100% (2)
- Hygiene and Sanitary Practices in The Fruit JuiceDocument19 pagesHygiene and Sanitary Practices in The Fruit JuiceJoyce Marian BelonguelNo ratings yet
- Dementia EssayDocument16 pagesDementia Essayscholify100% (1)
- Club FootDocument47 pagesClub FootSujanaNo ratings yet
- Pain Essay - What Are The Pathways Involved in The Sensation of Pain and How Can We Manipulate Them For Our BenefitDocument5 pagesPain Essay - What Are The Pathways Involved in The Sensation of Pain and How Can We Manipulate Them For Our BenefitscholifyNo ratings yet
- Mood Disorders Short EssayDocument4 pagesMood Disorders Short EssayscholifyNo ratings yet
- Animal Models Short Exam EssayDocument8 pagesAnimal Models Short Exam EssayscholifyNo ratings yet
- What Is The Neuropharmacological Basis of Drug Addiction II EssayDocument5 pagesWhat Is The Neuropharmacological Basis of Drug Addiction II EssayscholifyNo ratings yet
- The Role of Serotonin in Depression EssayDocument4 pagesThe Role of Serotonin in Depression EssayscholifyNo ratings yet
- Sound Localization EssayDocument11 pagesSound Localization EssayscholifyNo ratings yet
- Describe The Neural Mechanisms Underlying The Stretch Reflex. How Might This Contribute To The Control of Posture and Movement?Document3 pagesDescribe The Neural Mechanisms Underlying The Stretch Reflex. How Might This Contribute To The Control of Posture and Movement?scholifyNo ratings yet
- 1295188730neuro Essay 2 - Compare The Properties of Rods and Cones, and Their Retinal Pathways EssayDocument4 pages1295188730neuro Essay 2 - Compare The Properties of Rods and Cones, and Their Retinal Pathways EssayscholifyNo ratings yet
- Discuss The Drugs Used To Treat Depression EssayDocument9 pagesDiscuss The Drugs Used To Treat Depression EssayscholifyNo ratings yet
- Write An Essay On Schizophrenia and The Drugs That Can Be Used To Treat It IIDocument4 pagesWrite An Essay On Schizophrenia and The Drugs That Can Be Used To Treat It IIscholifyNo ratings yet
- Fillers and Vessels The Story of Arterial Obstruction After Cosmetic TreatmentDocument4 pagesFillers and Vessels The Story of Arterial Obstruction After Cosmetic TreatmentHerald Scholarly Open AccessNo ratings yet
- CAM ICU Training PDFDocument32 pagesCAM ICU Training PDFSabrinaMaharaniNo ratings yet
- Global Burden of Disease GBD Study 2017 18 PDFDocument70 pagesGlobal Burden of Disease GBD Study 2017 18 PDFtutagNo ratings yet
- ONGC Report First Pit Less Drilling in ONGC Scripts Success at RajahmundryDocument6 pagesONGC Report First Pit Less Drilling in ONGC Scripts Success at RajahmundryPETROPATH FLUIDS INDIA PVT. LTD.No ratings yet
- Biology Project SampleDocument30 pagesBiology Project SampleKen VargheseNo ratings yet
- Daftar Pustaka ImunologiDocument2 pagesDaftar Pustaka ImunologiJacklyn FultonNo ratings yet
- A Bill: in The House of RepresentativesDocument5 pagesA Bill: in The House of Representativesal mooreNo ratings yet
- AneurysmDocument22 pagesAneurysmRaymond SorianoNo ratings yet
- Blueprint For The Provision of Comprehensive Care For Trans Persons and Their Communities in The Caribbean and Other Anglophone CountriesDocument88 pagesBlueprint For The Provision of Comprehensive Care For Trans Persons and Their Communities in The Caribbean and Other Anglophone CountriesTRANScending BordersNo ratings yet
- GSK Consumer Healthcare Brands PortfolioDocument7 pagesGSK Consumer Healthcare Brands PortfolioSamarendra ChakrabortyNo ratings yet
- The New Nutrition Facts Label Examples of Different Label FormatsDocument16 pagesThe New Nutrition Facts Label Examples of Different Label Formatsice_coldNo ratings yet
- Parasitic WormsDocument4 pagesParasitic WormsEricNo ratings yet
- Prevention of Colon Polyps and CancerDocument3 pagesPrevention of Colon Polyps and CancerShrija DevendranNo ratings yet
- Bells PalsyDocument33 pagesBells PalsyzzakieNo ratings yet
- Chapter 01 - Introduction To DrugsDocument3 pagesChapter 01 - Introduction To DrugsDaniel BenitezNo ratings yet
- "Undifferentiated Schizophrenia": A Case Study OnDocument81 pages"Undifferentiated Schizophrenia": A Case Study OnHomework Ping100% (1)
- 2cmc ToR For Sewarage System Design AdamaDocument11 pages2cmc ToR For Sewarage System Design AdamaAnonymous 67xRG0eINNo ratings yet
- April 2017Document60 pagesApril 2017Treatment Plant Operator MagazineNo ratings yet