You might also like
- ATLS 8th EditionDocument50 pagesATLS 8th EditionPaolo VegaNo ratings yet
- Non Invasive Ventilation in PediatricsDocument192 pagesNon Invasive Ventilation in Pediatricstj1983tj0% (1)
- CXR Lecture DR Lenora FernandezDocument70 pagesCXR Lecture DR Lenora Fernandezapi-19431894100% (1)
- Optiflow Presentation-Carly TorgersenDocument12 pagesOptiflow Presentation-Carly Torgersenapi-252628311100% (1)
- Acutely Ill ChildDocument50 pagesAcutely Ill ChildAhmed KhanNo ratings yet
- Ccam N Bps Management PDFDocument9 pagesCcam N Bps Management PDFEthan AmalNo ratings yet
- Canadian Triage and Acuity Scale for PediatricsDocument30 pagesCanadian Triage and Acuity Scale for PediatricsPrince Jhessie L. AbellaNo ratings yet
- Initial Assessment and Management of Trauma PatientsDocument8 pagesInitial Assessment and Management of Trauma PatientsAlvin De LunaNo ratings yet
- NHS Lanarkshire Major Haemorrhage GuideDocument3 pagesNHS Lanarkshire Major Haemorrhage GuideleicesterbugNo ratings yet
- Initial Trauma Assessment GuideDocument5 pagesInitial Trauma Assessment GuidezulfahNo ratings yet
- Surgical Cricothyrotomy (Assist)Document5 pagesSurgical Cricothyrotomy (Assist)ydtrgnNo ratings yet
- Airway ManagementDocument63 pagesAirway ManagementGilang GumilangNo ratings yet
- 8.the Atls ProtocolDocument57 pages8.the Atls ProtocolReuben DutiNo ratings yet
- Pre-Op Preparation and Assessment of Pediatric PatientsDocument62 pagesPre-Op Preparation and Assessment of Pediatric PatientsBedahanakugmNo ratings yet
- Interpretation Chest X RayDocument127 pagesInterpretation Chest X RayVimal NishadNo ratings yet
- Air Leak SyndromesDocument2 pagesAir Leak SyndromesIchalAzNo ratings yet
- PICU Common ProblemDocument49 pagesPICU Common ProblemRawabi rawabi1997No ratings yet
- FOM Study Guide: Pleural Cavity, Lung Volumes & EffusionsDocument3 pagesFOM Study Guide: Pleural Cavity, Lung Volumes & EffusionsBernadine Cruz Par100% (1)
- Triage First Fast Track Guidelines 2Document14 pagesTriage First Fast Track Guidelines 2Bayu Wirantika0% (1)
- European Consensus On The Management of RDSDocument41 pagesEuropean Consensus On The Management of RDSDeddy Supriyadi100% (1)
- Intravenous Fluid Therapy in Critically Ill AdultsDocument17 pagesIntravenous Fluid Therapy in Critically Ill AdultsntnquynhproNo ratings yet
- Advances in Emergent Airway Management in PediatricsDocument19 pagesAdvances in Emergent Airway Management in PediatricsLuis Miguel VillanuevaNo ratings yet
- Gerry B. Acosta, MD, FPPS, FPCC: Pediatric CardiologistDocument51 pagesGerry B. Acosta, MD, FPPS, FPCC: Pediatric CardiologistChristian Clyde N. ApigoNo ratings yet
- ILS Case Studies COMP 2020.ppsxDocument39 pagesILS Case Studies COMP 2020.ppsxKim Orven KhoNo ratings yet
- Fetal, Transition and Neonatal Circulation: Divya Mishra Dept of PediatricsDocument37 pagesFetal, Transition and Neonatal Circulation: Divya Mishra Dept of PediatricsMathan KarthikNo ratings yet
- DR Lily - Resp Distress in Newborn Infants PDFDocument45 pagesDR Lily - Resp Distress in Newborn Infants PDFM Ilham MNo ratings yet
- Congenital Heart Disease ExplainedDocument74 pagesCongenital Heart Disease ExplainedKeith LajotNo ratings yet
- AnastesiDocument22 pagesAnastesidhitadwynNo ratings yet
- 3 Abdominal Ultrasound Imaging AnatomyDocument7 pages3 Abdominal Ultrasound Imaging Anatomyjefaturaimagenologia Hospital NogalarNo ratings yet
- Pediatrics ECG by DR Ali Bel KheirDocument9 pagesPediatrics ECG by DR Ali Bel KheirFerasNo ratings yet
- Kod - S Guide On Final Professional Exam 1 PDFDocument31 pagesKod - S Guide On Final Professional Exam 1 PDFHassanAbasNo ratings yet
- Chest Trauma: Annet Mary Mathew Anu Krishna Arathi.KDocument60 pagesChest Trauma: Annet Mary Mathew Anu Krishna Arathi.KAsif AbbasNo ratings yet
- Trauma Assessment: Aims of The Initial Evaluation of Trauma PatientsDocument6 pagesTrauma Assessment: Aims of The Initial Evaluation of Trauma Patientsece142No ratings yet
- Ob Rapid Response Team Plan1Document20 pagesOb Rapid Response Team Plan1api-255697457100% (1)
- Acute Limb IschaemiaDocument32 pagesAcute Limb IschaemiaAnonymous 9wHscM100% (1)
- Atrial Septial DefectDocument22 pagesAtrial Septial DefectJulie MckinneyNo ratings yet
- Arterial Puncture and CannulationDocument19 pagesArterial Puncture and CannulationAzizah Rahawarin100% (1)
- Newborn Respiratory Distress 11.28.2011Document41 pagesNewborn Respiratory Distress 11.28.2011Emily EresumaNo ratings yet
- Paediatric Emergencies NotesDocument6 pagesPaediatric Emergencies NotesJana AldourNo ratings yet
- Rational Blood Transfusion in Infant and ChildrenDocument37 pagesRational Blood Transfusion in Infant and ChildrenBayu KurniawanNo ratings yet
- PedsCases - Anaphylaxis Emergency TreatmentDocument5 pagesPedsCases - Anaphylaxis Emergency TreatmentSara Ilyas KhanNo ratings yet
- Eloesser Flap Thoracostomy WindowDocument20 pagesEloesser Flap Thoracostomy WindowJEFFRI JEFFRINo ratings yet
- Initial Assessment and Management: Presented by Fayez Abillama, MDDocument53 pagesInitial Assessment and Management: Presented by Fayez Abillama, MDDaniel GhosseinNo ratings yet
- Whitten - 2011 - Case Study - Reduced BiPAP Days - PM-185047373 - A PDFDocument3 pagesWhitten - 2011 - Case Study - Reduced BiPAP Days - PM-185047373 - A PDFdragon66No ratings yet
- Abdominal X RayDocument45 pagesAbdominal X RayAbdullah As'adNo ratings yet
- Contrast EchocardiographyDocument54 pagesContrast EchocardiographySruthiNo ratings yet
- Interpreting The Chest Radio Graph Friendly)Document9 pagesInterpreting The Chest Radio Graph Friendly)Vagner BorgesNo ratings yet
- Min Min Min Min: Most Urgent Very Urgent Urgent Less Urgent Not UrgentDocument1 pageMin Min Min Min: Most Urgent Very Urgent Urgent Less Urgent Not UrgentAlma Alnajjar0% (1)
- Causes Obstruction Causes CSF To Build Up in The Brain. If The Cause Is Congenital, Symptoms Such As AnDocument22 pagesCauses Obstruction Causes CSF To Build Up in The Brain. If The Cause Is Congenital, Symptoms Such As Anmhelandie100% (1)
- Nsg241 Study Guide Exam 5Document76 pagesNsg241 Study Guide Exam 5NatalieAndersonNo ratings yet
- Cardiac MonitorDocument4 pagesCardiac MonitorFahyesha MaulaniNo ratings yet
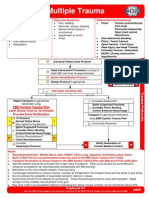
- Multiple Trauma ManagementDocument1 pageMultiple Trauma ManagementSetiawan Arif WibowoNo ratings yet
- In-Patient Department Staff & Bed DistributionDocument6 pagesIn-Patient Department Staff & Bed DistributionSiddhi RaneNo ratings yet
- Abdominal Tuberculosis: Causes, Symptoms and Imaging FindingsDocument111 pagesAbdominal Tuberculosis: Causes, Symptoms and Imaging Findingswasim siddiquiNo ratings yet
- Resusitasi NeonatusDocument22 pagesResusitasi NeonatusnikkitaihsanNo ratings yet
- Prehospital Anesthesia HandbookDocument46 pagesPrehospital Anesthesia HandbookoscarNo ratings yet
- Vascular Responses to PathogensFrom EverandVascular Responses to PathogensFelicity N.E. GavinsNo ratings yet