You might also like
- House Cleaning Estimate Sheet USDocument2 pagesHouse Cleaning Estimate Sheet USAlanNo ratings yet
- 2010 To 2011indmar Operators ManualDocument94 pages2010 To 2011indmar Operators Manualinforlex100% (3)
- Home Maint CojDocument41 pagesHome Maint Cojasti100% (2)
- QuickTIPS Sample Water Damage PaperworkDocument4 pagesQuickTIPS Sample Water Damage PaperworkMike SporNo ratings yet
- Work:: Daily Monday Tuesday Wednesday Thursday Friday SaturdayDocument4 pagesWork:: Daily Monday Tuesday Wednesday Thursday Friday Saturdaycoley31No ratings yet
- Hall PassDocument2 pagesHall PassEljun BaijamNo ratings yet
- Manual 2003 PresentwebDocument94 pagesManual 2003 PresentwebSerban Dinu BuligaNo ratings yet
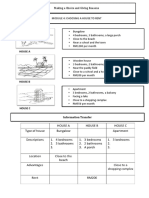
- Module4choosingahousetorentworksheets 140308191355 Phpapp02Document7 pagesModule4choosingahousetorentworksheets 140308191355 Phpapp02Darsenee RajaNo ratings yet
- Infant Daily ReportDocument2 pagesInfant Daily ReportRebecca Steele-MaffucciNo ratings yet
- Request For LeaveDocument1 pageRequest For Leavekmac87No ratings yet
- Casifmas Restorante Casifmas Restorante: Table Reservation Form Table Reservation FormDocument1 pageCasifmas Restorante Casifmas Restorante: Table Reservation Form Table Reservation FormrhodefrancestuazonNo ratings yet
- Request For LeaveDocument1 pageRequest For Leavekmac87100% (1)
- Check List For Residents MoveDocument1 pageCheck List For Residents Moveapi-262881860No ratings yet
- JLois Service and Accomplishment ReportDocument1 pageJLois Service and Accomplishment ReportMiles Dela CruzNo ratings yet
- Poultry Farm ChecklistDocument1 pagePoultry Farm ChecklistBernadette Lou LasinNo ratings yet
- Blank Monthly Work Calendar (2) 2Document1 pageBlank Monthly Work Calendar (2) 2Nikia DanielsNo ratings yet
- Kitchen Requirement FormDocument4 pagesKitchen Requirement Formroshini krishnaNo ratings yet
- 901366836394554219aho Seller Lead Source FormDocument3 pages901366836394554219aho Seller Lead Source FormRickNo ratings yet
- Participation SheetDocument1 pageParticipation SheetEladar LookNo ratings yet
- Design ProjectDocument18 pagesDesign Projectapi-524003828No ratings yet
- Kami Export - Microsoft Word - Rop Job Application With Availablity Front-For FillableDocument2 pagesKami Export - Microsoft Word - Rop Job Application With Availablity Front-For Fillableapi-459912383No ratings yet
- Slip Imus-StabDocument2 pagesSlip Imus-StabSonita VecinalNo ratings yet
- Notes Form 2-Pages-57-60Document4 pagesNotes Form 2-Pages-57-60api-299647607No ratings yet
- Buyer Lead SheetDocument2 pagesBuyer Lead SheetJustin CarruthNo ratings yet
- Event-Verification-Form 2Document1 pageEvent-Verification-Form 2api-600776345No ratings yet
- Microsoft Word 2 - Rop Job Application With Availablity Front-For FillableDocument2 pagesMicrosoft Word 2 - Rop Job Application With Availablity Front-For Fillableapi-356012886No ratings yet
- Planning: ..For The Enjoyment of Life!Document4 pagesPlanning: ..For The Enjoyment of Life!Anonymous yy8In96j0rNo ratings yet
- Restroom ChecklistDocument2 pagesRestroom ChecklistjhelNo ratings yet
- Camp Registration 2009Document1 pageCamp Registration 2009legacyofbob100% (1)
- Client FormsDocument5 pagesClient Formsapi-423121022No ratings yet
- Medication CardDocument2 pagesMedication CardNicole J. CastillejosNo ratings yet
- Bentons Week W EmilyDocument1 pageBentons Week W EmilyJennie Schooler-HamiltonNo ratings yet
- Property Listing TemplateDocument1 pageProperty Listing Templateneo9434No ratings yet
- Application of Mess OffDocument1 pageApplication of Mess OffaiwnwnsajNo ratings yet
- Microsoft Word - Rop Job Application With Availablity Front-For FillableDocument2 pagesMicrosoft Word - Rop Job Application With Availablity Front-For Fillableapi-355999946No ratings yet
- Restaurant Daily Performance ReportDocument3 pagesRestaurant Daily Performance ReportAqilahNo ratings yet
- Facility Use Request FormDocument2 pagesFacility Use Request Formsenai 2021No ratings yet
- Progress ReportDocument1 pageProgress ReportSVP KIDS ENGLISHNo ratings yet
- Rop Application: Directions: Please Print LegiblyDocument2 pagesRop Application: Directions: Please Print Legiblyapi-460266872No ratings yet
- Itinerary of TravelDocument1 pageItinerary of TravelBrgyTigbao CarLeyNo ratings yet
- Work For EnglishDocument2 pagesWork For Englishapi-403578194No ratings yet
- Inspection ChecklistDocument10 pagesInspection ChecklistJosiah CockroftNo ratings yet
- GUIA 8-11 Años JUNIOR 2Document31 pagesGUIA 8-11 Años JUNIOR 2iris machinNo ratings yet
- Activity Restaurant Comment CardDocument1 pageActivity Restaurant Comment CardEliza PicosNo ratings yet
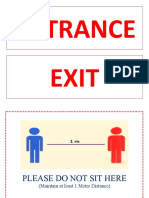
- Posters Please Do Not Sit HereDocument12 pagesPosters Please Do Not Sit HereRichelle MagpulongNo ratings yet
- Microsoft Word - Rop Job Application With Availablity Front-For FillableDocument2 pagesMicrosoft Word - Rop Job Application With Availablity Front-For Fillableapi-459942716No ratings yet
- NursingAssessmentForm - Nakita Pangestika - 3CDocument4 pagesNursingAssessmentForm - Nakita Pangestika - 3CEmi LestariNo ratings yet
- 4.operating Room RecordDocument1 page4.operating Room RecordDienizs LabiniNo ratings yet
- Client Satisfaction FormDocument1 pageClient Satisfaction FormYHONG SILVANONo ratings yet
- Total Bill Amount To Be Endorsed Total Bill Amount To Be EndorsedDocument1 pageTotal Bill Amount To Be Endorsed Total Bill Amount To Be EndorsedCeasar Ryan AsuncionNo ratings yet
- Application For Leave of AbsenceDocument1 pageApplication For Leave of AbsenceRoi Vince PiliNo ratings yet
- Testing Commisioning Report Water Softener: ProjectDocument1 pageTesting Commisioning Report Water Softener: Projectagun gunawanNo ratings yet
- Learner's Needs, Progress and Achievement CardexDocument3 pagesLearner's Needs, Progress and Achievement CardexJeremie Mariano AbanNo ratings yet
- Onsite Sewage Application For Approval FormDocument3 pagesOnsite Sewage Application For Approval FormtnedjoNo ratings yet
- Rop Job Application With Availability - Fillable For WebsiteDocument2 pagesRop Job Application With Availability - Fillable For Websiteapi-461364363No ratings yet
- InspectDocument1 pageInspectG-SamNo ratings yet
- Webelos Den Meeting PlanningDocument1 pageWebelos Den Meeting PlanningSelene ClarkNo ratings yet
- Daily Time Record: OUT IN OUT IN Remarks Date IN Lunch Break OUT RemarksDocument1 pageDaily Time Record: OUT IN OUT IN Remarks Date IN Lunch Break OUT RemarksBORDALLO JAYMHARKNo ratings yet
- Governmental Traumatizing Investigations: An Application to Get a New Toilet, Part IFrom EverandGovernmental Traumatizing Investigations: An Application to Get a New Toilet, Part INo ratings yet