You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Yoga - Asana Pranayama Mudra BandhaDocument567 pagesYoga - Asana Pranayama Mudra BandhaPravin Deshmukh100% (51)
- Ultimate Keto Guidebook 2023Document26 pagesUltimate Keto Guidebook 2023lhr11682No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- JLPeach Glute Guide v2Document4 pagesJLPeach Glute Guide v2Bárbara Leite33% (3)
- Nursing Care Plan For Alzheimer's DiseaseDocument4 pagesNursing Care Plan For Alzheimer's DiseaseRnspeakcom100% (1)
- Jurnal Manajemen Pelayanan KesehatanDocument5 pagesJurnal Manajemen Pelayanan KesehatanMohammad Rifqi WibowoNo ratings yet
- Colon PolypsDocument65 pagesColon PolypsorianattNo ratings yet
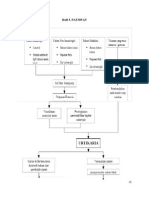
- Bab 3Document2 pagesBab 3Mohammad Rifqi WibowoNo ratings yet
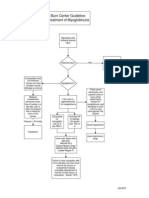
- A Flowchart of Treatment of Burn InjuryDocument1 pageA Flowchart of Treatment of Burn InjuryMohammad Rifqi WibowoNo ratings yet
- Myoglobin Uri ADocument1 pageMyoglobin Uri AMohammad Rifqi WibowoNo ratings yet
- Konsep Diri Dan StresDocument12 pagesKonsep Diri Dan StresMohammad Rifqi WibowoNo ratings yet
- Exstrophy and Epispadias MedscapeDocument18 pagesExstrophy and Epispadias MedscapeMohammad Rifqi WibowoNo ratings yet
- Summer Shred - Female Week 3Document36 pagesSummer Shred - Female Week 3Vincent CurcioNo ratings yet
- OIL OIL: Sonnenblumenöl SonnenblumenölDocument1 pageOIL OIL: Sonnenblumenöl Sonnenblumenölmanuel condreaNo ratings yet
- DIVORCE Sociology AssignmentDocument18 pagesDIVORCE Sociology AssignmentkeirenmavimbelaNo ratings yet
- Nutration For para Athletes-SportsDocument2 pagesNutration For para Athletes-SportsTavethiya MansukhNo ratings yet
- ESL PresentationDocument11 pagesESL PresentationNora LinNo ratings yet
- 309 2264 1 PBDocument6 pages309 2264 1 PBMatlubul KhairiNo ratings yet
- Exercise For Fitness: "Strengthen Your Faith Through Physical Exercise"Document19 pagesExercise For Fitness: "Strengthen Your Faith Through Physical Exercise"Goodness- Gabihan, IyannaNo ratings yet
- Free Workout Plan MenDocument7 pagesFree Workout Plan MenAli SarooshNo ratings yet
- The Change Plan - w1Document2 pagesThe Change Plan - w1ruziyanaNo ratings yet
- Self Regulation 04Document3 pagesSelf Regulation 04Shahadath Hossain HimelNo ratings yet
- Food Biotechnology Sports NutritionDocument14 pagesFood Biotechnology Sports NutritionAngelo PalmeroNo ratings yet
- Maintining A Safe and Sustainable Exercise ProgramDocument7 pagesMaintining A Safe and Sustainable Exercise ProgramMary Delle JamolaonNo ratings yet
- Physical Education Health1Document23 pagesPhysical Education Health1Victorio PeronahackangfirstaccountNo ratings yet
- RandomDocument2 pagesRandomDavid SanjuNo ratings yet
- Understanding The Self by Prof. Jennifer T. Composa (For Instructional Purposes Only) The Material SelfDocument38 pagesUnderstanding The Self by Prof. Jennifer T. Composa (For Instructional Purposes Only) The Material SelfXedric AlvarezNo ratings yet
- Chapter 5 Childhood ElderlyDocument24 pagesChapter 5 Childhood Elderlyr55fsf75hpNo ratings yet
- Excercise 2 Activity 7 DoniDocument6 pagesExcercise 2 Activity 7 DoniDoni SaragihNo ratings yet
- Healthy Eating Thesis StatementDocument5 pagesHealthy Eating Thesis Statementqrikaiiig100% (2)
- Complete Programming and Periodization For Hypertrophy Training - How To Write A Hypertrophy ProgramDocument3 pagesComplete Programming and Periodization For Hypertrophy Training - How To Write A Hypertrophy ProgramWaldir Martins NetoNo ratings yet
- Assessments CH 13 NutritionDocument23 pagesAssessments CH 13 NutritionIman HusainatNo ratings yet
- Prescribing An Annual Plan For The Competitive.3Document10 pagesPrescribing An Annual Plan For The Competitive.3Scott_PTNo ratings yet
- Misfit Phase 3 Guide and Checkin - 4Document3 pagesMisfit Phase 3 Guide and Checkin - 4hmimezNo ratings yet
- NCP - Imbalanced NutritionDocument3 pagesNCP - Imbalanced NutritionRay Daniel E. BilbaoNo ratings yet
- Effects of Sprint Interval Training and Body.24Document8 pagesEffects of Sprint Interval Training and Body.24Maxwell MartinsNo ratings yet
- Circuit Training For Fat LossDocument2 pagesCircuit Training For Fat LossRico martin OsoNo ratings yet
- Bridging The Digital Divide in Health Care The Role of HIT in Addressing Racial and Ethnic DisparitiesDocument9 pagesBridging The Digital Divide in Health Care The Role of HIT in Addressing Racial and Ethnic DisparitiesArjun YadavNo ratings yet