You might also like
- Orthodontic Consent FormDocument3 pagesOrthodontic Consent FormDiana Suharti100% (1)
- Psychiatry Board Examination: ST U D Y Gu Id E F O R T HeDocument502 pagesPsychiatry Board Examination: ST U D Y Gu Id E F O R T HeMandeep morNo ratings yet
- Capnography - Self Study - GuideDocument22 pagesCapnography - Self Study - GuideSuresh KumarNo ratings yet
- Vindicate For LBPDocument10 pagesVindicate For LBPShaun TylerNo ratings yet
- Crash RespiratoryDocument245 pagesCrash Respiratoryridin007100% (5)
- Med NotesDocument6 pagesMed NotesNeva CarpioNo ratings yet
- Case History, MSE and Rating Scales - in Psychological AssessmentDocument29 pagesCase History, MSE and Rating Scales - in Psychological Assessmentsu84No ratings yet
- Part III Internal Medicine Examination AnswersDocument91 pagesPart III Internal Medicine Examination AnswersFırat GüllüNo ratings yet
- Respiratory Assessment GuidelinesDocument1 pageRespiratory Assessment GuidelinesAmeliaM100% (2)
- Clinical Pearls in Pulmonology (2018) PDFDocument183 pagesClinical Pearls in Pulmonology (2018) PDFCristinaLucanNo ratings yet
- Ophelia'S Case: Oleh: Anggun Fitri Utami, S, Ked PembimbingDocument20 pagesOphelia'S Case: Oleh: Anggun Fitri Utami, S, Ked PembimbingAnggun Cimey UtamiNo ratings yet
- Pulmonology - Study Guide PDFDocument77 pagesPulmonology - Study Guide PDFDanielle Groupfive100% (2)
- Bronchiectasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandBronchiectasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Spirometry in PracticeDocument24 pagesSpirometry in Practiceuser_at_scribd100% (1)
- Airway Clearance Techniques and Hyperinflation Therapy Walsh Chapter 12Document25 pagesAirway Clearance Techniques and Hyperinflation Therapy Walsh Chapter 12Dennis Páez Torres100% (2)
- Valvular Heart Disease: Presented by DR Mirjana Milutinovic Professor, SJSMDocument69 pagesValvular Heart Disease: Presented by DR Mirjana Milutinovic Professor, SJSMAbanoub AwadallaNo ratings yet
- Clinical Examination A Systematic Guide To Physical Diagnosis by Nicholas J Talley Simon Ox00027connor B00ib1kza0Document5 pagesClinical Examination A Systematic Guide To Physical Diagnosis by Nicholas J Talley Simon Ox00027connor B00ib1kza0Hitna hitnaNo ratings yet
- Interpretting ABG SuccessfullyDocument15 pagesInterpretting ABG Successfullyanimathz100% (1)
- Cardiology Ebook Notes PDFDocument26 pagesCardiology Ebook Notes PDFsugisweNo ratings yet
- Aortic Regurgitation CaseDocument38 pagesAortic Regurgitation CaseIka MagfirahNo ratings yet
- Pulmonary Patho PDFDocument623 pagesPulmonary Patho PDFNabeel Shahzad100% (1)
- Respiratory ExaminationDocument20 pagesRespiratory ExaminationAmirul SyafizNo ratings yet
- Personal History: Notes in Clinical CardiologyDocument19 pagesPersonal History: Notes in Clinical CardiologyRachitha GuttaNo ratings yet
- Respiratory Notes (Chris Andersen, ICUPrimaryPrep - Com)Document14 pagesRespiratory Notes (Chris Andersen, ICUPrimaryPrep - Com)PkernNo ratings yet
- CHFDocument20 pagesCHFdistihardiyanti100% (1)
- S1 and S2: Valves) at The Start of The Systolic Contraction of The VentriclesDocument10 pagesS1 and S2: Valves) at The Start of The Systolic Contraction of The VentriclesCHARIEMAE CA�AZARESNo ratings yet
- Core V - Cardiovascular CoreDocument35 pagesCore V - Cardiovascular CoreMatthew LeiNo ratings yet
- Final PhysioDocument1,111 pagesFinal PhysioSana Savana Aman R100% (1)
- Pediatric Cardiology LectureDocument87 pagesPediatric Cardiology LectureMena HashemNo ratings yet
- Pulmonary Rehabilitation Information: Dr. Deepak Talwar Best Lung Specialist in DelhiDocument16 pagesPulmonary Rehabilitation Information: Dr. Deepak Talwar Best Lung Specialist in DelhiMetro HospitalNo ratings yet
- Heart Sounds: Mitral Regurgitation Congestive Heart FailureDocument6 pagesHeart Sounds: Mitral Regurgitation Congestive Heart FailurecindyNo ratings yet
- One Stop Doc Immunology - Stewart, John, Sadler, AmyDocument153 pagesOne Stop Doc Immunology - Stewart, John, Sadler, AmyCosmin NeaguNo ratings yet
- History Taking and Physical Examination of Cardiovascular System-The EssentialsDocument72 pagesHistory Taking and Physical Examination of Cardiovascular System-The EssentialsReena Joanella TimbreNo ratings yet
- 7th Heart Sounds and MurmursDocument6 pages7th Heart Sounds and MurmursbabibubeboNo ratings yet
- CVS-01 Examination & Short CasesDocument9 pagesCVS-01 Examination & Short Casesem khanNo ratings yet
- Chronic Obstructive Lung Diseases and Chronic Restrictive Lung DiseasesDocument59 pagesChronic Obstructive Lung Diseases and Chronic Restrictive Lung DiseasesGEORGENo ratings yet
- Chest Pain PresentationDocument24 pagesChest Pain PresentationAnonymous 17awurSUNo ratings yet
- Ischemic Heart Disease Notes AtfDocument23 pagesIschemic Heart Disease Notes AtfSingha ChangsiriwatanaNo ratings yet
- Acid Base ImbalanceDocument50 pagesAcid Base ImbalanceDian Pratiwi BurnamaNo ratings yet
- UVA Surgical Clerkship Survival GuideDocument15 pagesUVA Surgical Clerkship Survival GuideNadiim Rajabalee100% (1)
- ANAT2341 Embryology: Early and Systemic Development: School of Medical SciencesDocument8 pagesANAT2341 Embryology: Early and Systemic Development: School of Medical SciencesJimson EchaveNo ratings yet
- OutputDocument12 pagesOutputzenishzalamNo ratings yet
- Approach: A. How The Kidney Handle The Proteins?Document9 pagesApproach: A. How The Kidney Handle The Proteins?Rashed ShatnawiNo ratings yet
- ABG AnalysisDocument22 pagesABG Analysisrajan40dmcNo ratings yet
- CNS ProformaDocument8 pagesCNS Proformaamogh anandNo ratings yet
- Angiology NoteDocument13 pagesAngiology NoteSantosh Bhandari100% (2)
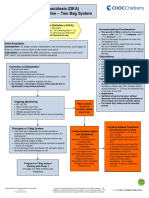
- Diabetic Ketoacidosis Care GuidelineDocument5 pagesDiabetic Ketoacidosis Care GuidelineRahma DhNo ratings yet
- Adult Chest X-RayDocument60 pagesAdult Chest X-RayAnil DasNo ratings yet
- Current News in CardiologyDocument428 pagesCurrent News in CardiologyDenisa DiaconuNo ratings yet
- Heart SoundsDocument4 pagesHeart SoundsAthie100% (1)
- Main DivisionDocument61 pagesMain DivisionChadCowgillNo ratings yet
- Lung Pathology Flow ChartsDocument6 pagesLung Pathology Flow ChartsZagros Motamed100% (1)
- Davies Veterinary Specialists UnderstandingDocument3 pagesDavies Veterinary Specialists UnderstandingFelicity HumphreysNo ratings yet
- Tracheostomy: ENT Department DMC & Hospital Ludhiana PunjabDocument46 pagesTracheostomy: ENT Department DMC & Hospital Ludhiana PunjabVikrant MittalNo ratings yet
- Pulmonology Short CasesDocument10 pagesPulmonology Short CasesRZ Ng100% (1)
- Lung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesFrom EverandLung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesAlain JunodNo ratings yet
- The Audio PANCE and PANRE Episode 9Document4 pagesThe Audio PANCE and PANRE Episode 9The Physician Assistant Life100% (1)
- Keith Hopcroft - Instant Wisdom For GPs - Pearls From All The Specialities-CRC Press (2024)Document274 pagesKeith Hopcroft - Instant Wisdom For GPs - Pearls From All The Specialities-CRC Press (2024)Adil Abdul SalamNo ratings yet
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Star Health and Allied Insurance Company Limited: Prospectus - Mediclassic Insurance Policy (Individual)Document8 pagesStar Health and Allied Insurance Company Limited: Prospectus - Mediclassic Insurance Policy (Individual)mfsrajNo ratings yet
- Bipolar DisorderDocument8 pagesBipolar DisorderJan Elishah Camarador AllareyNo ratings yet
- Utah KidneyDocument16 pagesUtah KidneyChristineGonzalesNo ratings yet
- The Use and Function of The SettingDocument5 pagesThe Use and Function of The SettingFruzsee89No ratings yet
- Revalida Review NotesDocument14 pagesRevalida Review NotesBryan Lloyd RayatNo ratings yet
- 1 de Jesus v. Employees CompensationDocument6 pages1 de Jesus v. Employees CompensationCAJNo ratings yet
- Enfermedades Emergentes y Embarazo - EID - November 2006 - Volume CompletoDocument187 pagesEnfermedades Emergentes y Embarazo - EID - November 2006 - Volume CompletoRuth Vargas GonzalesNo ratings yet
- Interstitial NephritisDocument2 pagesInterstitial NephritisYosi Dwi Saputro Part IINo ratings yet
- Venous Blood Gas (VBG) PDFDocument3 pagesVenous Blood Gas (VBG) PDFZamzam DomaNo ratings yet
- MEROPENEMDocument4 pagesMEROPENEMfurqan ahmadNo ratings yet
- Treatments For Mental Illness TimelineaDocument5 pagesTreatments For Mental Illness TimelineanesumaNo ratings yet
- BronchiolitisDocument45 pagesBronchiolitisYuusuf MubarikNo ratings yet
- Star Comprehensive Policy Clause New 1Document16 pagesStar Comprehensive Policy Clause New 1Manu SNo ratings yet
- Herniated Nucleus PulposusDocument13 pagesHerniated Nucleus PulposusLorebell100% (4)
- Drug Study (Lactulose, Zynapse, Simvastatin) and HTP - CVD Prob CardioembolismDocument9 pagesDrug Study (Lactulose, Zynapse, Simvastatin) and HTP - CVD Prob CardioembolismRene John FranciscoNo ratings yet
- A Rare Case of Acute Abdomen: DR - Rajeev Thilak C, DR - Ramadoss.P, DR - Ameesh Izath, DR - Christianne SandhyaDocument3 pagesA Rare Case of Acute Abdomen: DR - Rajeev Thilak C, DR - Ramadoss.P, DR - Ameesh Izath, DR - Christianne SandhyaRajeev ThilakNo ratings yet
- Diagnosis Penyakit Dalam Bahasa InggrisDocument10 pagesDiagnosis Penyakit Dalam Bahasa InggrisPutri Sulung WidodoNo ratings yet
- Dissociative Identity Disorder A Pathophysiological PhenomenonDocument3 pagesDissociative Identity Disorder A Pathophysiological PhenomenonArhip CojocNo ratings yet
- What Is Autism Spectrum Disorder?Document17 pagesWhat Is Autism Spectrum Disorder?Mark HibionadaNo ratings yet
- NOte BookDocument81 pagesNOte BookDr abdiaziz osman JamaNo ratings yet
- 2023.jama - ICardíaca Con FEVI Preservada PDFDocument12 pages2023.jama - ICardíaca Con FEVI Preservada PDFEmanuelNo ratings yet
- Verb Tense - StructureDocument3 pagesVerb Tense - Structureapi-179604969No ratings yet
- Actaapa 2018 21Document5 pagesActaapa 2018 21Argitya RighoNo ratings yet
- RCH PALS Study Guide - Web-121514Document5 pagesRCH PALS Study Guide - Web-121514Ryan N Brandy CooperNo ratings yet
- Ari WhoDocument55 pagesAri WholingghezhiNo ratings yet
- Module 21 - Health, Stress, and CopingDocument53 pagesModule 21 - Health, Stress, and CopingDo Kyungsooooo100% (1)
- 1.who Shall Be Considered As Having Community-Acquired Pneumonia?Document6 pages1.who Shall Be Considered As Having Community-Acquired Pneumonia?Kristine Jade OdtujanNo ratings yet
- Standardization, Development and Organoleptic Evaluation of Nutri Bar Supplemented With Barley (Hordeum Vulgare)Document5 pagesStandardization, Development and Organoleptic Evaluation of Nutri Bar Supplemented With Barley (Hordeum Vulgare)Abu Sufiyan FarooquiNo ratings yet