You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Home Health Services Coverage and Limitations Handbook - AdoptionDocument104 pagesHome Health Services Coverage and Limitations Handbook - AdoptionRad EkkawiNo ratings yet
- Textbook For Mrcog 1 by Richa Saxena 9385891286Document5 pagesTextbook For Mrcog 1 by Richa Saxena 9385891286DrMuhammad Hassan50% (2)
- LOPADocument84 pagesLOPAM100% (4)
- Final Sop Manual-1-1Document62 pagesFinal Sop Manual-1-1Dianne JoyNo ratings yet
- Big Blue Miller 700Document98 pagesBig Blue Miller 700Juan Eduardo JeRico100% (1)
- 1 Fee Structure For Regular Students 22 23Document1 page1 Fee Structure For Regular Students 22 23Haseeb BuzdarNo ratings yet
- Harga Jual - XLSX - Sheet1Document13 pagesHarga Jual - XLSX - Sheet1HADI PRAYITNONo ratings yet
- Tle9 Agricrop q2 m1 Handlingmaterialsequipment v2Document32 pagesTle9 Agricrop q2 m1 Handlingmaterialsequipment v2Bernadeth Torres LibradoNo ratings yet
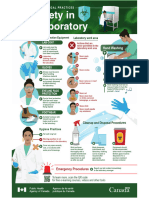
- Biosafety in The LaboratoryDocument1 pageBiosafety in The LaboratoryALFARO CHAT CARMINA ROSARIONo ratings yet
- Awareness On Comprehensive Sexuality Education Among Junior High School Teacherstowards The Designing of Teacher'S Training ModulesDocument9 pagesAwareness On Comprehensive Sexuality Education Among Junior High School Teacherstowards The Designing of Teacher'S Training ModulesJulia Mar Antonete Tamayo AcedoNo ratings yet
- Labrep. 1Document6 pagesLabrep. 1Joy MananganNo ratings yet
- Lingual-Keys For SuccessDocument8 pagesLingual-Keys For SuccessGoutam NookalaNo ratings yet
- Promissory Note Promissory Note: Mauban District Hospital Mauban District HospitalDocument2 pagesPromissory Note Promissory Note: Mauban District Hospital Mauban District HospitalKC PalattaoNo ratings yet
- Light 27 Web FinalDocument28 pagesLight 27 Web FinalrafilhouseNo ratings yet
- Atlanticare TQM Implementation Case StudyDocument16 pagesAtlanticare TQM Implementation Case Study6132 PRINCE KUMARNo ratings yet
- Inpharmation February 2013Document16 pagesInpharmation February 2013ChemistixNo ratings yet
- Material Safety Data Sheet: I. General InformationDocument7 pagesMaterial Safety Data Sheet: I. General InformationPemalang HockNo ratings yet
- Working at Height TrainingDocument47 pagesWorking at Height TrainingthinkpadNo ratings yet
- Oral Hygiene InstructionsDocument20 pagesOral Hygiene Instructionsapi-307943695No ratings yet
- DBL Group TPWL Water Reuse System at Industrial ScaleDocument15 pagesDBL Group TPWL Water Reuse System at Industrial ScaleNavid ZamanNo ratings yet
- Chapter 2: Gerontological NursingDocument14 pagesChapter 2: Gerontological Nursingaznknight323100% (1)
- Elder AbuseDocument18 pagesElder Abusehermione1402No ratings yet
- Ten Personality Disorders - Neel Burton MDDocument11 pagesTen Personality Disorders - Neel Burton MDcgarciNo ratings yet
- Safety Campaign-Bypassing Safety Control-Feb 2022Document4 pagesSafety Campaign-Bypassing Safety Control-Feb 2022HSE99 BHDCNo ratings yet
- GHMC ABC VetDocument2 pagesGHMC ABC VetApril SamaNo ratings yet
- 58 - Towards A Philosophy of Public HealthDocument7 pages58 - Towards A Philosophy of Public HealthprabowoNo ratings yet
- HEARTDocument11 pagesHEART1NC21IS038 POLATHALA MOUNIKANo ratings yet
- Assignment On Decision Making ProcessDocument23 pagesAssignment On Decision Making ProcessMuhammad SaeedNo ratings yet
- Thesis Topics For Construction Project ManagementDocument7 pagesThesis Topics For Construction Project Managementbsqbr7px100% (1)
- Vitamin K: Adjunct To Vitamin DDocument7 pagesVitamin K: Adjunct To Vitamin DBeena WalvekarNo ratings yet