You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Assessment CenterDocument23 pagesAssessment Centerliferocks232No ratings yet
- Washington State Ombudsman Investigation of Colville Child Welfare Office, 2009Document86 pagesWashington State Ombudsman Investigation of Colville Child Welfare Office, 2009Rick ThomaNo ratings yet
- A Solid Waste Management Survey in Davao Del Sur (School and Household Waste Management Survey)Document6 pagesA Solid Waste Management Survey in Davao Del Sur (School and Household Waste Management Survey)LY SA Amurao IINo ratings yet
- Appendix A Listing of FormsDocument2 pagesAppendix A Listing of FormsRick ThomaNo ratings yet
- Elliott-2017-Journal of Nursing ManagementDocument5 pagesElliott-2017-Journal of Nursing Managementprofesi nersNo ratings yet
- Interim Chief Executive Officer in United States Resume John WinengerDocument2 pagesInterim Chief Executive Officer in United States Resume John WinengerJohnWinengerNo ratings yet
- Aparchit Super Ga Paid Booster For Rbi Grade B & Idbi Excutive PDFDocument724 pagesAparchit Super Ga Paid Booster For Rbi Grade B & Idbi Excutive PDFAstricNo ratings yet
- 1110 Fin3119 Risk and InsuranceDocument5 pages1110 Fin3119 Risk and InsuranceDadink Dunkers Part IINo ratings yet
- UB-04 Billing Instructions Revision Table: Revision Date Sections Revised DescriptionDocument24 pagesUB-04 Billing Instructions Revision Table: Revision Date Sections Revised DescriptioncmabryNo ratings yet
- Direct Marketing Department, Central Office, YogakshemaDocument9 pagesDirect Marketing Department, Central Office, YogakshematsrajanNo ratings yet
- Frauds and ScamsDocument100 pagesFrauds and ScamsSunil Rawat100% (1)
- Master Auditing Document Draft With Secondary Responses - SQF Level IIDocument95 pagesMaster Auditing Document Draft With Secondary Responses - SQF Level IIFloreid100% (1)
- HR PoliciesDocument127 pagesHR Policiesmuthuswamy77No ratings yet
- Order of Appointment Dermatology and Skin Cancer Center of South Carolina SignedDocument4 pagesOrder of Appointment Dermatology and Skin Cancer Center of South Carolina SignedWMBF NewsNo ratings yet
- Proiect Buss - Int.Document31 pagesProiect Buss - Int.Stanciu MihaelaNo ratings yet
- Democrats Abroad LCC 2015 AGM Minutes FINALDocument4 pagesDemocrats Abroad LCC 2015 AGM Minutes FINALCarmelan PolceNo ratings yet
- Tomalon Residence - Floor Plan - 2021202-ARCHTLjkghjfjfDocument1 pageTomalon Residence - Floor Plan - 2021202-ARCHTLjkghjfjfEdg ManapolNo ratings yet
- PRAB Agenda Nov 2017Document5 pagesPRAB Agenda Nov 2017City of Boulder ColoradoNo ratings yet
- Healthcare Facilities in Emerging Countries The Challenge For IndiaDocument140 pagesHealthcare Facilities in Emerging Countries The Challenge For Indiapino panoNo ratings yet
- Resume Shanae18 - CCBCDocument2 pagesResume Shanae18 - CCBCapi-412903421No ratings yet
- Notice of Privacy Practices (Generic)Document3 pagesNotice of Privacy Practices (Generic)cecilled_08No ratings yet
- Payslip - Dec 16-31, 2020 - RLCDocument15 pagesPayslip - Dec 16-31, 2020 - RLCKassandra faith jewel alabatNo ratings yet
- Emergency Action PlanDocument3 pagesEmergency Action PlanAlexanderthethirdNo ratings yet
- PESTEL AnalysisDocument2 pagesPESTEL AnalysisCarly Greatrex50% (2)
- California Fire Siege 2003 - The StoryDocument99 pagesCalifornia Fire Siege 2003 - The StorySouthern California Public RadioNo ratings yet
- Notification OBC PO and AO PostsDocument10 pagesNotification OBC PO and AO PostsAnil NegiNo ratings yet
- MCK Petitions Done, Eir in Works: Ad Iver NionDocument10 pagesMCK Petitions Done, Eir in Works: Ad Iver NionMad River UnionNo ratings yet
- ACCOMPLISHMENT REPORT ON PRACTICUM ACTIVITIES - Week 1 (AutoRecovered)Document10 pagesACCOMPLISHMENT REPORT ON PRACTICUM ACTIVITIES - Week 1 (AutoRecovered)Narahmie RuadoNo ratings yet
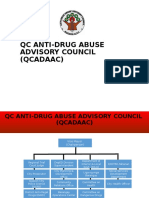
- QC QCPD Anti-Drug Abuse Advisory Council (QCADAAC)Document17 pagesQC QCPD Anti-Drug Abuse Advisory Council (QCADAAC)Minnie Agdeppa50% (2)