You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- F - Issue 197F - Issue 197Document116 pagesF - Issue 197F - Issue 197Petr Švarc38% (8)
- Bruce Lee ArticleDocument4 pagesBruce Lee ArticlePetr ŠvarcNo ratings yet
- Original Tao Inward Training PDFDocument294 pagesOriginal Tao Inward Training PDFPetr Švarc100% (3)
- Bruce Lee ArticleDocument4 pagesBruce Lee ArticlePetr ŠvarcNo ratings yet
- Fighting Words: Douglas WileDocument21 pagesFighting Words: Douglas WilePetr ŠvarcNo ratings yet
- 34 IYFTCCA JournalDocument102 pages34 IYFTCCA JournalPetr Švarc100% (2)
- Zhu Xi's Spiritual Practice As The Basis of His Central Philosophical ConceptsDocument37 pagesZhu Xi's Spiritual Practice As The Basis of His Central Philosophical ConceptsnahualpaNo ratings yet
- Taiji Teoreticka Cast 2Document5 pagesTaiji Teoreticka Cast 2Petr Švarc100% (2)
- MTJ SP12 BodyMechanicsDocument5 pagesMTJ SP12 BodyMechanicsPetr ŠvarcNo ratings yet
- The Red Book Photos: Dong (Tung) Family Taijiquan Long Form Photographs of Tung Ying ChiehDocument34 pagesThe Red Book Photos: Dong (Tung) Family Taijiquan Long Form Photographs of Tung Ying ChiehДориян Александров100% (1)
- Taiji Teoreticka Cast 1Document11 pagesTaiji Teoreticka Cast 1Petr Švarc100% (2)
- Tao of BodyDocument193 pagesTao of BodyPetr Švarc100% (19)
- Tao of BodyDocument193 pagesTao of BodyPetr Švarc100% (19)
- Fascial Fitness Training in The Neuromyofascial WebDocument11 pagesFascial Fitness Training in The Neuromyofascial Webgavinbroomes100% (1)
- Science and Cvilization in China - Part 5Document608 pagesScience and Cvilization in China - Part 5Petr Švarc100% (1)
- Moseley 2012 PAIN MANAGEMDocument3 pagesMoseley 2012 PAIN MANAGEMPetr Švarc100% (1)
- Hsing-I - Robert SmithDocument110 pagesHsing-I - Robert Smithviki100% (21)
- 13 Forem MecDocument1 page13 Forem MecPetr ŠvarcNo ratings yet
- BaihuiDocument1 pageBaihuiPetr ŠvarcNo ratings yet
- Contoh Label Sensus 2022Document313 pagesContoh Label Sensus 2022Ajenk SablackNo ratings yet
- Puratattva No 41Document3 pagesPuratattva No 41ultimategoonNo ratings yet
- FoundationDocument98 pagesFoundationManognya KotaNo ratings yet
- GoodElearning TOGAF Poster 46 - Adapting The ADMDocument1 pageGoodElearning TOGAF Poster 46 - Adapting The ADMFabian HidalgoNo ratings yet
- Assignment 5 WarehousingDocument4 pagesAssignment 5 WarehousingabbasNo ratings yet
- Using Impact IX49 and 61 With Nektar DAW Integration 1.1Document21 pagesUsing Impact IX49 and 61 With Nektar DAW Integration 1.1Eko SeynNo ratings yet
- GARCH (1,1) Models: Ruprecht-Karls-Universit at HeidelbergDocument42 pagesGARCH (1,1) Models: Ruprecht-Karls-Universit at HeidelbergRanjan KumarNo ratings yet
- Pre Intermediate Talking ShopDocument4 pagesPre Intermediate Talking ShopSindy LiNo ratings yet
- Methods of Estimation For Building WorksDocument22 pagesMethods of Estimation For Building Worksvara prasadNo ratings yet
- Backward Forward PropogationDocument19 pagesBackward Forward PropogationConrad WaluddeNo ratings yet
- Design of CouplingDocument75 pagesDesign of CouplingVatsal BhalaniNo ratings yet
- The Adoption of e Procurement in Tanzani PDFDocument5 pagesThe Adoption of e Procurement in Tanzani PDFDangyi GodSeesNo ratings yet
- Zoom g2 1nu Manual Do Utilizador PDFDocument56 pagesZoom g2 1nu Manual Do Utilizador PDFEliude Gonçalves FerreiraNo ratings yet
- Logarithms Functions: Background Information Subject: Grade Band: DurationDocument16 pagesLogarithms Functions: Background Information Subject: Grade Band: DurationJamaica PondaraNo ratings yet
- Power - Factor - Correction - LegrandDocument24 pagesPower - Factor - Correction - LegrandrehanNo ratings yet
- Bosch Injectors and OhmsDocument6 pagesBosch Injectors and OhmsSteve WrightNo ratings yet
- IDL6543 ModuleRubricDocument2 pagesIDL6543 ModuleRubricSteiner MarisNo ratings yet
- Tree Based Machine Learning Algorithms Decision Trees Random Forests and Boosting B0756FGJCPDocument109 pagesTree Based Machine Learning Algorithms Decision Trees Random Forests and Boosting B0756FGJCPJulio Davalos Vasquez100% (1)
- Information Brochure: (Special Rounds)Document35 pagesInformation Brochure: (Special Rounds)Praveen KumarNo ratings yet
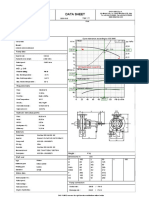
- Data Sheet: Item N°: Curve Tolerance According To ISO 9906Document3 pagesData Sheet: Item N°: Curve Tolerance According To ISO 9906Aan AndianaNo ratings yet
- Hayek - Planning, Science, and Freedom (1941)Document5 pagesHayek - Planning, Science, and Freedom (1941)Robert Wenzel100% (1)
- Huawei Switch - Service - ConfigDocument5 pagesHuawei Switch - Service - ConfigTranHuuPhuocNo ratings yet
- Changing Historical Perspectives On The Nazi DictatorshipDocument9 pagesChanging Historical Perspectives On The Nazi Dictatorshipuploadimage666No ratings yet
- Postmodernism in Aha! MovieDocument2 pagesPostmodernism in Aha! MovieSayma AkterNo ratings yet
- Assistant Bookkeeper Resume Sample - Best Format - Great Sample ResumeDocument4 pagesAssistant Bookkeeper Resume Sample - Best Format - Great Sample ResumedrustagiNo ratings yet
- PhotometryDocument2 pagesPhotometryHugo WNo ratings yet
- Florida Motor Fuel Tax Relief Act of 2022Document9 pagesFlorida Motor Fuel Tax Relief Act of 2022ABC Action NewsNo ratings yet
- ARCASIA Students Design Competition TORDocument4 pagesARCASIA Students Design Competition TORDeena McgeeNo ratings yet
- Excavation Trench Permit Ex 1 F0206Document5 pagesExcavation Trench Permit Ex 1 F0206emeka2012No ratings yet
- 13 SK Kader Pendamping PGSDocument61 pages13 SK Kader Pendamping PGSrachman ramadhanaNo ratings yet