You might also like
- Encyclopedia of Women's HealthDocument717 pagesEncyclopedia of Women's HealthSenia Dzwoneczek Žarković100% (4)
- Gender Differences in Mental HealthDocument7 pagesGender Differences in Mental HealthpentagonNo ratings yet
- Consent Guidelines 15012013Document12 pagesConsent Guidelines 15012013Blue SunNo ratings yet
- Hum - Gender Inequality and Health of Women Some Socio-Cultural IssuesDocument6 pagesHum - Gender Inequality and Health of Women Some Socio-Cultural IssuesImpact JournalsNo ratings yet
- Barenreiter CatalogDocument60 pagesBarenreiter CatalogAndrea Rovati0% (2)
- SeawaterDocument9 pagesSeawaterBlue SunNo ratings yet
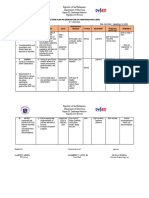
- Action Plan ESP 2023 24Document2 pagesAction Plan ESP 2023 24Je-Ann EstriborNo ratings yet
- BSP Accomplishment Report SampleDocument3 pagesBSP Accomplishment Report SampleMelbourneSinisin83% (6)
- Dying to Count: Post-Abortion Care and Global Reproductive Health Politics in SenegalFrom EverandDying to Count: Post-Abortion Care and Global Reproductive Health Politics in SenegalNo ratings yet
- Article On 1970s Angola Mercenaries, Colonel Mad Dog Callan Etc PDFDocument8 pagesArticle On 1970s Angola Mercenaries, Colonel Mad Dog Callan Etc PDFNick MustNo ratings yet
- Health Care Challenges in IndiaDocument8 pagesHealth Care Challenges in IndiaKailash NagarNo ratings yet
- Vital Signs: The Deadly Costs of Health InequalityFrom EverandVital Signs: The Deadly Costs of Health InequalityRating: 4 out of 5 stars4/5 (1)
- Rainbow Grade R BIG Book 1 2015 ResizedDocument22 pagesRainbow Grade R BIG Book 1 2015 ResizedLaurelleNo ratings yet
- Health and Medicine Write-UpDocument16 pagesHealth and Medicine Write-UpZIMBO MUSIC ENTERTAINMENT TVNo ratings yet
- 30.08.22 - All Medicine Is SocialDocument4 pages30.08.22 - All Medicine Is SocialPola PhotographyNo ratings yet
- Ahs - 547B (Unit-Iii & Iv) Cultural Disease and IllnessDocument8 pagesAhs - 547B (Unit-Iii & Iv) Cultural Disease and IllnessSakshi GargNo ratings yet
- Medical SociologyDocument25 pagesMedical SociologyHajra MirzaNo ratings yet
- 06 - Chapter 2 PDFDocument38 pages06 - Chapter 2 PDFSuraj DubeyNo ratings yet
- Unit 5 PDFDocument14 pagesUnit 5 PDFGurpreet KaurNo ratings yet
- Gender HealthDocument7 pagesGender Healthneelam handikherkarNo ratings yet
- International Encyclopedia of The Social and Behavioral Sciences, Elsevier Science LTD.Document11 pagesInternational Encyclopedia of The Social and Behavioral Sciences, Elsevier Science LTD.Khirod Chandra MoharanaNo ratings yet
- The Politics of Potential: Global Health and Gendered Futures in South AfricaFrom EverandThe Politics of Potential: Global Health and Gendered Futures in South AfricaNo ratings yet
- Psychopathology in Women: Incorporating Gender Perspective into Descriptive PsychopathologyFrom EverandPsychopathology in Women: Incorporating Gender Perspective into Descriptive PsychopathologyMargarita Sáenz-HerreroNo ratings yet
- Intern Med, Vol. 6, 2006, Pp. 667-669. 10.1111/j.1525-1497.2006.0512.xDocument1 pageIntern Med, Vol. 6, 2006, Pp. 667-669. 10.1111/j.1525-1497.2006.0512.xOmer KhanNo ratings yet
- Reflection PaperDocument7 pagesReflection Paperapi-572962598No ratings yet
- Social Class & Health Status: EssayDocument6 pagesSocial Class & Health Status: EssayRavi Mana-ay EjarNo ratings yet
- Social Exclusion Caste Health - A Review Based On The SocialDocument9 pagesSocial Exclusion Caste Health - A Review Based On The SocialSanthosh TekumalNo ratings yet
- Paper 11 PDFDocument186 pagesPaper 11 PDFK K SHUKLANo ratings yet
- Understanding Health, Medicine, and SocietyDocument5 pagesUnderstanding Health, Medicine, and SocietySummer DavzNo ratings yet
- Origins of Ayurveda Have Been Traced To Around 6,000Document13 pagesOrigins of Ayurveda Have Been Traced To Around 6,000PriyankaNo ratings yet
- Notes For TestDocument44 pagesNotes For TestJingosi RAMPHARWANENo ratings yet
- 19 and 20 Social Patterning of Health and IllnessDocument61 pages19 and 20 Social Patterning of Health and IllnessLucy EvrettNo ratings yet
- Calling Family: Digital Technologies and the Making of Transnational Care CollectivesFrom EverandCalling Family: Digital Technologies and the Making of Transnational Care CollectivesNo ratings yet
- Running Head: Importance of Medical Sociology 1Document2 pagesRunning Head: Importance of Medical Sociology 1George Herbert ModyNo ratings yet
- Final Chep 1Document5 pagesFinal Chep 1api-578023155No ratings yet
- Instructor Marked Excercice HLSCDocument13 pagesInstructor Marked Excercice HLSCJuanQuinteroNo ratings yet
- Medical Anthropology NoteDocument37 pagesMedical Anthropology NoteKeyeron DugumaNo ratings yet
- Östlin - Paying Attention To GenderDocument6 pagesÖstlin - Paying Attention To GendermariaconstanzavasqueNo ratings yet
- LC459 CW1 SOH (Jubair) (Feedback)Document10 pagesLC459 CW1 SOH (Jubair) (Feedback)Death StrokeNo ratings yet
- 1 Medical Sociology LectureDocument36 pages1 Medical Sociology LectureBrain RunnerNo ratings yet
- PubHealth DOAJScieloDocument10 pagesPubHealth DOAJScieloBernadeta Setyo VenantiNo ratings yet
- The Social Phenomenon of Arthritis As A Chronic Disease in Relation To The FamilyDocument6 pagesThe Social Phenomenon of Arthritis As A Chronic Disease in Relation To The FamilyNiranjala GamageNo ratings yet
- Clinical Lessons From Anthropologic and Cross-Cultural ResearchDocument11 pagesClinical Lessons From Anthropologic and Cross-Cultural ResearchmohdrusydiNo ratings yet
- Medical Sociology 3Document7 pagesMedical Sociology 3Manav VyasNo ratings yet
- Exploring New Horizons: Medical Anthropology in Public HealthDocument6 pagesExploring New Horizons: Medical Anthropology in Public Healthibnu cahyonoNo ratings yet
- Depression and Health Seeking BehaviorDocument6 pagesDepression and Health Seeking BehaviorVictor MangomaNo ratings yet
- PracheeY. Health&Wellbeing EssayDocument4 pagesPracheeY. Health&Wellbeing Essayjulyyy105No ratings yet
- Key Issues: What Is HEALTH?Document5 pagesKey Issues: What Is HEALTH?Kenneth ColeNo ratings yet
- AHS 547B (Unit4) Sakshi Garg MSC 4thDocument5 pagesAHS 547B (Unit4) Sakshi Garg MSC 4thSakshi GargNo ratings yet
- FinalDocument15 pagesFinalapi-275091887No ratings yet
- SOSC 3169 EXAM PREP BY Muhammed SyedDocument8 pagesSOSC 3169 EXAM PREP BY Muhammed SyedmuhammedNo ratings yet
- Gender and Health - The Effects of Constrained Choices and Social Policies (PDFDrive)Document317 pagesGender and Health - The Effects of Constrained Choices and Social Policies (PDFDrive)Iness Billyon34No ratings yet
- Chapter 2 Q&ADocument2 pagesChapter 2 Q&AYyCNo ratings yet
- Health Literacy On Hypertension and Functional Health Status Among Elderly of Malabon City, PhilippinesDocument20 pagesHealth Literacy On Hypertension and Functional Health Status Among Elderly of Malabon City, PhilippinesGlobal Research and Development ServicesNo ratings yet
- Structural Competency in Mental Health and Medicine: A Case-Based Approach to Treating the Social Determinants of HealthFrom EverandStructural Competency in Mental Health and Medicine: A Case-Based Approach to Treating the Social Determinants of HealthNo ratings yet
- Assignment 1 Social ScienceDocument3 pagesAssignment 1 Social ScienceGela ReyesNo ratings yet
- Hps 439a Final Paper 1Document9 pagesHps 439a Final Paper 1api-280707253No ratings yet
- Amar Jesani On Understanding Health Book ReviewDocument3 pagesAmar Jesani On Understanding Health Book ReviewAmar JesaniNo ratings yet
- Society and Culture.: HCD 1123: Introduction To Basic Sociology and AnthropologyDocument13 pagesSociety and Culture.: HCD 1123: Introduction To Basic Sociology and AnthropologyDeborah moraaNo ratings yet
- Amar Jesani: Violence and Health Care Profession in IndiaDocument13 pagesAmar Jesani: Violence and Health Care Profession in IndiaAmar JesaniNo ratings yet
- ROLE OF SOCIOLOGY IN HEALTH FinalDocument2 pagesROLE OF SOCIOLOGY IN HEALTH FinalaminaNo ratings yet
- AssignmentDocument4 pagesAssignmentManvi RiddhiNo ratings yet
- HSH207 ThiThuyTrangLY AT1Document9 pagesHSH207 ThiThuyTrangLY AT1Huong NguyenNo ratings yet
- Great Compassion Mantra A Nagy Együttérzés MantrájaDocument1 pageGreat Compassion Mantra A Nagy Együttérzés MantrájaBlue SunNo ratings yet
- How Do People Inherit AlphaDocument1 pageHow Do People Inherit AlphaBlue SunNo ratings yet
- General Anatomy: Epithelial TissueDocument22 pagesGeneral Anatomy: Epithelial TissueBlue SunNo ratings yet
- Full TextDocument3 pagesFull TextBlue SunNo ratings yet
- Sidang Ilahi Elohim Dalam Mazmur 82:1: Marthin Steven Lumingkewas & Firman PanjaitanDocument25 pagesSidang Ilahi Elohim Dalam Mazmur 82:1: Marthin Steven Lumingkewas & Firman PanjaitanDoni MarpaungNo ratings yet
- Objective of Child ActDocument10 pagesObjective of Child ActjoancelestNo ratings yet
- Costco Objectives InvestigationDocument6 pagesCostco Objectives InvestigationlinsssNo ratings yet
- One Summer Night: Ambrose BierceDocument7 pagesOne Summer Night: Ambrose Bierce恩洁白No ratings yet
- Class#2 FSA - Level 1 To Be - Dick-Vilchez-GarcìaDocument7 pagesClass#2 FSA - Level 1 To Be - Dick-Vilchez-GarcìaFernanda CastroNo ratings yet
- Confucius IntroDocument7 pagesConfucius IntroMarcio TrabassoNo ratings yet
- Cifra Club - Billie Eilish - Billie Bossa NovaDocument3 pagesCifra Club - Billie Eilish - Billie Bossa NovaAmanda MirandaNo ratings yet
- NIM ScheduleDocument2 pagesNIM SchedulePrabh SinghNo ratings yet
- Si3586DV: Vishay SiliconixDocument13 pagesSi3586DV: Vishay SiliconixLeslie StewartNo ratings yet
- Accounting For Overheads by DR Kamlesh KhoslaDocument16 pagesAccounting For Overheads by DR Kamlesh KhoslaKrati SinghalNo ratings yet
- External Whistleblowing ProceduresDocument9 pagesExternal Whistleblowing Proceduresgautham kannanNo ratings yet
- Airworthiness Directive: Number: Ata: Effective Date: Type Certificate: SubjectDocument2 pagesAirworthiness Directive: Number: Ata: Effective Date: Type Certificate: SubjectBahadorNo ratings yet
- Word OrderDocument6 pagesWord OrderEditura Sf MinaNo ratings yet
- Claridge Apartments Co. v. Commissioner of Internal RevenueDocument20 pagesClaridge Apartments Co. v. Commissioner of Internal RevenueScribd Government DocsNo ratings yet
- 184 People v. de La CruzDocument2 pages184 People v. de La CruzPatricia Kaye O. SevillaNo ratings yet
- Alcantara Vs de VeraDocument7 pagesAlcantara Vs de VeraRoanne May Manalo-SoriaoNo ratings yet
- r220 1Document216 pagesr220 1Mark CheneyNo ratings yet
- Iqbal and Muslim Renaissance - Business RecorderDocument5 pagesIqbal and Muslim Renaissance - Business Recorderiqra aftabNo ratings yet
- PMOB AllDocument300 pagesPMOB AllshashankNo ratings yet
- SAMRO Membership RequirementsDocument1 pageSAMRO Membership RequirementsSAMRO100% (3)
- Therapearl v. Veridian - 1st Amended ComplaintDocument39 pagesTherapearl v. Veridian - 1st Amended ComplaintSarah BursteinNo ratings yet
- Environmental ClearanceDocument5 pagesEnvironmental ClearanceRadhakrishnaNo ratings yet
- BackgroundDocument8 pagesBackgroundhey lucy!No ratings yet
- Determining The Benefits of Using Profanity in Expressing Emotions of Grade 12 Students in FCICDocument5 pagesDetermining The Benefits of Using Profanity in Expressing Emotions of Grade 12 Students in FCICPaola CalunsagNo ratings yet
- Pres en Tors CourtDocument6 pagesPres en Tors CourtJess BrighamNo ratings yet
- DDMA Order No 373 DT 15.04.3021Document7 pagesDDMA Order No 373 DT 15.04.3021The Indian Express92% (13)