You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
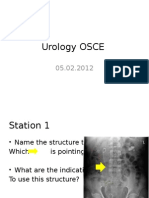
- Urology OSCEDocument9 pagesUrology OSCEJihad Anad75% (4)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Diagnostic Microbiology in Antibiotic PolicyDocument46 pagesDiagnostic Microbiology in Antibiotic Policytummalapalli venkateswara raoNo ratings yet
- Student Exploration: Human KaryotypingDocument5 pagesStudent Exploration: Human KaryotypingTurkan Amirova75% (4)
- ANZAA Apheresis Education Guidelines Jun01Document14 pagesANZAA Apheresis Education Guidelines Jun01Vonny Nurmalya MegawatiNo ratings yet
- Literature ReviewDocument3 pagesLiterature Reviewapi-610273615No ratings yet
- Done MDR RESEARCH PAPER With Fixed BordersDocument20 pagesDone MDR RESEARCH PAPER With Fixed BordersZoe MagnoNo ratings yet
- Executive Summary of UPenn OMFS Covid Conference - Indrakanti PDFDocument8 pagesExecutive Summary of UPenn OMFS Covid Conference - Indrakanti PDFasda201487No ratings yet
- Mary Clare Higgins-Chen, MD, MPH Donna Windish, MD, MPH: Alopecia Week 25Document9 pagesMary Clare Higgins-Chen, MD, MPH Donna Windish, MD, MPH: Alopecia Week 25omegasauron0gmailcomNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care Planapi-309251523No ratings yet
- Importance of ICT in Transport and CommunicationDocument3 pagesImportance of ICT in Transport and CommunicationSheikh FahadNo ratings yet
- IFU1062 Celosia Covered Stent Rev. BDocument11 pagesIFU1062 Celosia Covered Stent Rev. BAnnie NguyễnNo ratings yet
- Animal Care Policy ManualDocument42 pagesAnimal Care Policy ManualQueremosabarrabás A BarrabásNo ratings yet
- Evidence Based Interventions For NasDocument9 pagesEvidence Based Interventions For Nasapi-316356010No ratings yet
- Clinical Cheat Sheet: Radiographic AssessmentDocument1 pageClinical Cheat Sheet: Radiographic AssessmentTracy PopeNo ratings yet
- WJG 23 6137Document16 pagesWJG 23 6137MUHAMMAD09No ratings yet
- Informational Interview PaperDocument5 pagesInformational Interview Paperapi-525644495No ratings yet
- Traditional Treatment of Leucoderma by Kol Tribes of Vindhyan Region of Uttar PradeshDocument2 pagesTraditional Treatment of Leucoderma by Kol Tribes of Vindhyan Region of Uttar PradeshloNo ratings yet
- Amanda Haynes Revised ResumeDocument2 pagesAmanda Haynes Revised Resumeapi-300845540No ratings yet
- EB Neuro - STM9000 Products Line PDFDocument36 pagesEB Neuro - STM9000 Products Line PDFMuhamad wahyu Riansyah100% (1)
- CV KPM Jan 2020Document13 pagesCV KPM Jan 2020Prof. Dr. Kamlesh MehtaNo ratings yet
- DipiroDocument2 pagesDipiroFitriahzainNo ratings yet
- NCP Ortho WardDocument2 pagesNCP Ortho WardAira MaeNo ratings yet
- Understanding The Pathophysiology of Fever.45Document2 pagesUnderstanding The Pathophysiology of Fever.45drdion mangku alamNo ratings yet
- NCPDocument5 pagesNCPf_jm06_gNo ratings yet
- 647 4385 1 PB1 PDFDocument198 pages647 4385 1 PB1 PDFioko iokovNo ratings yet
- 7th Edition NRP Brings Big Changes For NRP Instructors: Instructor UpdateDocument12 pages7th Edition NRP Brings Big Changes For NRP Instructors: Instructor UpdateJoev SaquinNo ratings yet
- SaheliDocument4 pagesSaheliamar_vs2005No ratings yet
- Typhoid Fever para PresentDocument23 pagesTyphoid Fever para PresentGino Al Ballano BorinagaNo ratings yet
- The Annual Production Cycle For Influenza Vaccine: Catherine GerdilDocument4 pagesThe Annual Production Cycle For Influenza Vaccine: Catherine GerdilAntonio MoncayoNo ratings yet
- Dialysis and Disasters PresentationDocument21 pagesDialysis and Disasters Presentationapi-24755251No ratings yet