You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Odontogenic TumorsDocument32 pagesOdontogenic Tumorssatya_mds100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Cysts of The JawsDocument75 pagesCysts of The JawsSwetha KaripineniNo ratings yet
- Dentigerous CystDocument16 pagesDentigerous CystMudjiono MudjionoNo ratings yet
- Odontogenik Tumor JinakDocument130 pagesOdontogenik Tumor JinakAstrid Bernadette Ulina PurbaNo ratings yet
- MCQ Final 1984Document19 pagesMCQ Final 1984JohnSonNo ratings yet
- cysts 1-مدمجDocument306 pagescysts 1-مدمجأمال داودNo ratings yet
- نماذج اورال باثوDocument73 pagesنماذج اورال باثوReham ShehadaNo ratings yet
- Clasification of Odontogenic Tumours A ReviewDocument6 pagesClasification of Odontogenic Tumours A ReviewJuan Carlos MeloNo ratings yet
- JaypeeDigital - Ebook ReaderDocument40 pagesJaypeeDigital - Ebook ReaderHanin AbukhiaraNo ratings yet
- MCQ Final 1800Document19 pagesMCQ Final 1800JohnSonNo ratings yet
- Radiography Jaw LesionsDocument19 pagesRadiography Jaw LesionssrikantnairNo ratings yet
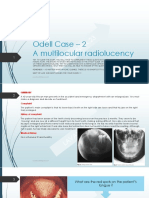
- Odell Case 2Document17 pagesOdell Case 2Anuradha KarriNo ratings yet
- Oral Pathology Revision 2010: By: Dr. Sahar El SheikhDocument211 pagesOral Pathology Revision 2010: By: Dr. Sahar El SheikhNada MohammedNo ratings yet
- Oral Pathology - Case Study 1 - FinalDocument5 pagesOral Pathology - Case Study 1 - Finalapi-262534732No ratings yet
- Oral MedicineDocument75 pagesOral MedicineAyush SoniNo ratings yet
- Proposal Karya Tulis AkhirDocument35 pagesProposal Karya Tulis Akhirredy pristantoNo ratings yet
- 11-Odontogenic Tumours 2Document118 pages11-Odontogenic Tumours 2Ash ArmyNo ratings yet
- Case #1: Case Study Assignment Assignment #3Document10 pagesCase #1: Case Study Assignment Assignment #3api-536664543No ratings yet
- Oral Radiology Principles and Interpretation 7th Ed PDFDocument14 pagesOral Radiology Principles and Interpretation 7th Ed PDFLaura Victoria Alvarez RodriguezNo ratings yet
- Ameloblastoma of The Jaw and Maxillary Bone: Clinical Study and Report of Our ExperienceDocument7 pagesAmeloblastoma of The Jaw and Maxillary Bone: Clinical Study and Report of Our ExperienceKharismaNisaNo ratings yet
- Contemporary Treatment of AmeloblastomaDocument7 pagesContemporary Treatment of AmeloblastomaomeerulrafieNo ratings yet
- Radiographic Analysis of Ameloblastoma: A Retrospective StudyDocument9 pagesRadiographic Analysis of Ameloblastoma: A Retrospective StudyhasnaNo ratings yet
- Differential Diagnosis - NewDocument11 pagesDifferential Diagnosis - NewMøĦãmèd Gämãl GømǮãNo ratings yet
- OrtodontieDocument33 pagesOrtodontieStefana NanuNo ratings yet
- GhgfdsDocument4 pagesGhgfdsUser NameNo ratings yet
- Scientific Programme BookletDocument44 pagesScientific Programme BookletPreetam PatnalaNo ratings yet
- Fibrosseus LesionDocument66 pagesFibrosseus LesionBhupinder KaushalNo ratings yet
- Jaw Tumours: Dr. Shabin Fahad Dept. of General SurgeryDocument16 pagesJaw Tumours: Dr. Shabin Fahad Dept. of General SurgeryGana ShettyNo ratings yet
- Odontogenic Tumors IIDocument24 pagesOdontogenic Tumors IIIbn HabibNo ratings yet
- CH15 Patho D&R AgamDocument11 pagesCH15 Patho D&R AgamBio CheNo ratings yet