You might also like
- MKT 6080 Final Project Milestone 2 WorksheetDocument12 pagesMKT 6080 Final Project Milestone 2 WorksheetDEENo ratings yet
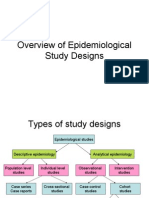
- Overview of Epidemiological Study DesignsDocument16 pagesOverview of Epidemiological Study DesignsLakshmi Seth100% (2)
- Arcon Vs Non Arcon Articulators.: Presented by Dr. Jeewan Bachan Dhinsa 1718703Document18 pagesArcon Vs Non Arcon Articulators.: Presented by Dr. Jeewan Bachan Dhinsa 1718703manasviNo ratings yet
- Wiley - Clinical Cases in Orthodontics - 978-1-118-29247-1Document2 pagesWiley - Clinical Cases in Orthodontics - 978-1-118-29247-1MayerNo ratings yet
- 1975 Jan-Feb #62Document28 pages1975 Jan-Feb #62Merlin ChowkwanyunNo ratings yet
- Leukoplakia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandLeukoplakia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Kim Seol Hee, 2019, The Effects of Orofacial Myofunctional Training On The PDFDocument9 pagesKim Seol Hee, 2019, The Effects of Orofacial Myofunctional Training On The PDFSerina Cahya NabilahNo ratings yet
- Review FrenectomyDocument6 pagesReview FrenectomyNyitnyit KunyitNo ratings yet
- Myofunctional Appliance Treatment: Sleep Dentistry For The 21st CenturyDocument4 pagesMyofunctional Appliance Treatment: Sleep Dentistry For The 21st CenturyNaeem MoollaNo ratings yet
- Periodicity DentalGuideDocument52 pagesPeriodicity DentalGuideSalam BataienehNo ratings yet
- Traumatic Injuries To The Teeth4541Document114 pagesTraumatic Injuries To The Teeth4541Irfan AliNo ratings yet
- Chapter 41.Ppt HypersensitivityDocument63 pagesChapter 41.Ppt HypersensitivityMaria Mercedes LeivaNo ratings yet
- Fluids and Electrolytes 2015Document117 pagesFluids and Electrolytes 2015Rashed ShatnawiNo ratings yet
- Good Morning.: @areebazainabDocument42 pagesGood Morning.: @areebazainabshabana waniNo ratings yet
- Minor Oral Surgical Procedures in Children ClassDocument65 pagesMinor Oral Surgical Procedures in Children ClassReenaChauhanNo ratings yet
- Medical Emergencies in The Dental Office PDFDocument52 pagesMedical Emergencies in The Dental Office PDFsrprior100% (1)
- Management of Class II Div IDocument13 pagesManagement of Class II Div Iapi-19840404No ratings yet
- Tanvi Shah - Maaz ShaikhDocument29 pagesTanvi Shah - Maaz ShaikhTanvi ShahNo ratings yet
- Prosthetic Management of Soft Palate Defects: Presented byDocument57 pagesProsthetic Management of Soft Palate Defects: Presented byPiyush DongreNo ratings yet
- Oral Manifestaions of Systemic DiseasesDocument116 pagesOral Manifestaions of Systemic DiseaseslikhithaNo ratings yet
- Pulp Therapy of Non-Vital Teeth (Pulpectomy)Document27 pagesPulp Therapy of Non-Vital Teeth (Pulpectomy)Mahmoud A. ZoghborNo ratings yet
- A Critical Appraisal of Tongue-Thrusting-Tulley PDFDocument11 pagesA Critical Appraisal of Tongue-Thrusting-Tulley PDFmalifaragNo ratings yet
- Extraoral and Intraoral ExaminationDocument64 pagesExtraoral and Intraoral ExaminationAhmed HotiebaNo ratings yet
- Manual CariogramDocument51 pagesManual CariogramDesty DarmaNo ratings yet
- Thumb Sucking HabbitDocument23 pagesThumb Sucking Habbitmabds312No ratings yet
- Secondary Bone Grafting For Alveolar Clefts SurgicalDocument6 pagesSecondary Bone Grafting For Alveolar Clefts SurgicalRidwan SNo ratings yet
- Periodontal Diseases in Children PedoDocument34 pagesPeriodontal Diseases in Children PedoFourthMolar.comNo ratings yet
- Periodontal Problems in KidsDocument49 pagesPeriodontal Problems in KidsRaksmey PhanNo ratings yet
- Existing Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDocument47 pagesExisting Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDaniel WangNo ratings yet
- Evaluation of The Relationship Between Bruxism and Premature Occlusal ContactsDocument6 pagesEvaluation of The Relationship Between Bruxism and Premature Occlusal ContactsWellyAnggarani100% (1)
- Epidemiologi Dental CariesDocument21 pagesEpidemiologi Dental CariesSampahAjaNo ratings yet
- NSAIDs in DentistryDocument7 pagesNSAIDs in DentistryEliza DNNo ratings yet
- Non-Caries Dental DiseaseDocument61 pagesNon-Caries Dental Diseaseapi-19916399No ratings yet
- DR Nick Lekic - Space MaintainersDocument35 pagesDR Nick Lekic - Space MaintainersanatomimanusiaNo ratings yet
- Administration of Coagulation-Altering Therapy in The Patient Presenting For Oral Health and Maxillofacial SurgeryDocument18 pagesAdministration of Coagulation-Altering Therapy in The Patient Presenting For Oral Health and Maxillofacial SurgeryLaura Giraldo QuinteroNo ratings yet
- Management of Pediatric Medical - Emergencies in The Dental OfficeDocument22 pagesManagement of Pediatric Medical - Emergencies in The Dental Officebanyubiru0% (1)
- Odontogenic Cysts Summary Chart: Radicular Cyst (Periapical Cyst)Document4 pagesOdontogenic Cysts Summary Chart: Radicular Cyst (Periapical Cyst)ML90No ratings yet
- Space Maintenance: Emma Laing, Paul Ashley, Farhad B. Naini & Daljit S. GillDocument8 pagesSpace Maintenance: Emma Laing, Paul Ashley, Farhad B. Naini & Daljit S. GillAnonymous JR1VNCNo ratings yet
- IRTDocument2 pagesIRTIgnacioNo ratings yet
- Tooth Discolour at Ion PedoDocument28 pagesTooth Discolour at Ion PedoFourthMolar.comNo ratings yet
- Crossbite PosteriorDocument11 pagesCrossbite PosteriorrohmatuwidyaNo ratings yet
- SSCDocument50 pagesSSCMustafa Tambawala100% (1)
- Dental Anatomy and PhysiologyDocument36 pagesDental Anatomy and PhysiologyCpt.WnchstrNo ratings yet
- D-Dentin-Lec 1Document45 pagesD-Dentin-Lec 1api-3710331100% (7)
- Association Between Oral Habits, Mouth BreathingDocument9 pagesAssociation Between Oral Habits, Mouth BreathingdewiayuNo ratings yet
- 2 Anatomy of TMJDocument117 pages2 Anatomy of TMJSugandhi Pidaparthi100% (1)
- CementumDocument10 pagesCementumAshish BisaneNo ratings yet
- Endodontics in Systemically Compromised PatientsDocument30 pagesEndodontics in Systemically Compromised Patientscarolina pavezNo ratings yet
- Space ManagementDocument11 pagesSpace Managementdr parveen bathla100% (1)
- Adpied Paper From EmailDocument17 pagesAdpied Paper From Emailapi-401213596No ratings yet
- Pulpectomy PedoDocument30 pagesPulpectomy PedoDr.Harsh100% (1)
- Dry Mouth (Xerostomia)Document18 pagesDry Mouth (Xerostomia)dr_jamal1983No ratings yet
- Impression Making - BDJ - 4800516aDocument9 pagesImpression Making - BDJ - 4800516aDr Anand Rajapur100% (1)
- Reducing The Risk of Failure Incomplete Denture PatientsDocument8 pagesReducing The Risk of Failure Incomplete Denture PatientsHisyam IshakNo ratings yet
- Avulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The ToothDocument39 pagesAvulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The Toothshailesh_shenoyNo ratings yet
- Lesions of Oral Soft Tissues in Children PedoDocument74 pagesLesions of Oral Soft Tissues in Children PedoFourthMolar.comNo ratings yet
- 2 Anatomical LandmarksDocument9 pages2 Anatomical LandmarksShady MahmoudNo ratings yet
- Dentin HypersenstivityDocument4 pagesDentin Hypersenstivitymohamed saadNo ratings yet
- 2dev of MaxillaDocument78 pages2dev of MaxillapriyaNo ratings yet
- Animal DentistryDocument10 pagesAnimal DentistryFei Fei LoNo ratings yet
- Access To Special Care Dentistry, Part 9. Special Care Dentistry Services For Older PeopleDocument14 pagesAccess To Special Care Dentistry, Part 9. Special Care Dentistry Services For Older PeoplehaihaitakNo ratings yet
- Revised Application Form PDFDocument1 pageRevised Application Form PDFDilmohit SinghNo ratings yet
- Infant Oral Health 1Document19 pagesInfant Oral Health 1Dilmohit SinghNo ratings yet
- Definition of Early Childhood Caries (ECC) : Originating Council Review Council Adopted RevisedDocument1 pageDefinition of Early Childhood Caries (ECC) : Originating Council Review Council Adopted RevisedDilmohit SinghNo ratings yet
- CGHS Bengaluru Rates List As On NOv.2014Document53 pagesCGHS Bengaluru Rates List As On NOv.2014mamuhydNo ratings yet
- Tooth BleachingDocument24 pagesTooth BleachingDilmohit SinghNo ratings yet
- PEAK Restoration of The Endodontically Treated ToothDocument20 pagesPEAK Restoration of The Endodontically Treated Toothlishenwong100% (1)
- Dentin BondingDocument15 pagesDentin BondingDilmohit SinghNo ratings yet
- 8.review Meenu Mary PaulDocument10 pages8.review Meenu Mary PaulDilmohit SinghNo ratings yet
- Bite SplintsDocument15 pagesBite SplintsAmit Parmar100% (1)
- FINAL SplintingDocument46 pagesFINAL SplintingDilmohit SinghNo ratings yet
- Perio TestDocument9 pagesPerio TestDilmohit SinghNo ratings yet
- Perio TestDocument9 pagesPerio TestDilmohit SinghNo ratings yet
- Reimplantation of Avulsed Primary IncisorsDocument4 pagesReimplantation of Avulsed Primary IncisorsDilmohit SinghNo ratings yet
- 53867257Document7 pages53867257Dilmohit SinghNo ratings yet
- Lingual Frenectomy Using Multiple Series Z-PlastyDocument3 pagesLingual Frenectomy Using Multiple Series Z-PlastyDilmohit SinghNo ratings yet
- A Carbohydrate-Restrictive Strategy Is Safer and As Efficient As Intensive Insulin Therapy in Critically Ill PatientsDocument6 pagesA Carbohydrate-Restrictive Strategy Is Safer and As Efficient As Intensive Insulin Therapy in Critically Ill PatientsTeresaNo ratings yet
- Health Optimizing Physical Education 1Document22 pagesHealth Optimizing Physical Education 1Russel MejicoNo ratings yet
- Department of Education: Action Plan For Wins (Wash in School)Document3 pagesDepartment of Education: Action Plan For Wins (Wash in School)Rosalie Belaguas Rojonan50% (2)
- 2005 PDFDocument436 pages2005 PDFAbdulazizNo ratings yet
- Group Mediclaim Policy Coverages For Employees of Century PlyDocument2 pagesGroup Mediclaim Policy Coverages For Employees of Century PlyUDAYNo ratings yet
- Practical Cardio-Oncology (2019, CRC Press)Document261 pagesPractical Cardio-Oncology (2019, CRC Press)Anitei GabrielaNo ratings yet
- Science 9 Quarter 1 Week 2 Sim 3Document30 pagesScience 9 Quarter 1 Week 2 Sim 3Jelly FloresNo ratings yet
- SpondylolisthesisDocument121 pagesSpondylolisthesisWilliam Surya HartantoNo ratings yet
- Test Bank For 3 2 1 Code It 2020 8th Edition Michelle Green Full DownloadDocument24 pagesTest Bank For 3 2 1 Code It 2020 8th Edition Michelle Green Full Downloadrobertabergmjnxqrasct100% (43)
- Hyperthermia HIV NURSING CARE PLAN FLODocument4 pagesHyperthermia HIV NURSING CARE PLAN FLOMicaela CrisostomoNo ratings yet
- Residency Prog CanadaDocument116 pagesResidency Prog Canadahswami20037730No ratings yet
- ABCDE Assessment Exam: Eunice QuijanoDocument3 pagesABCDE Assessment Exam: Eunice QuijanoQuijano GpokskieNo ratings yet
- Lectura Unidad 8Document16 pagesLectura Unidad 8Day FuNo ratings yet
- Gems and Gems Advanced 2016Document2 pagesGems and Gems Advanced 2016Plate MealsNo ratings yet
- Murshidabad Action Plan10-11Document13 pagesMurshidabad Action Plan10-11Prabir Kumar ChatterjeeNo ratings yet
- Uro-Gynaecology From Cambridge To UAE?Document28 pagesUro-Gynaecology From Cambridge To UAE?Michelle FynesNo ratings yet
- Contraindications To Implant Treatment 1Document1 pageContraindications To Implant Treatment 1Hussien A. Abu OlbaNo ratings yet
- Marshall Islands Medical Certificate B-SideDocument1 pageMarshall Islands Medical Certificate B-Sidedeniss sumilovsNo ratings yet
- Post Term PregnancyDocument22 pagesPost Term PregnancyDarianne HernandezNo ratings yet
- KMPDU Private Practice CBA EldoretDocument57 pagesKMPDU Private Practice CBA Eldoretapi-175531574No ratings yet
- Blood Glucose MonitoringDocument4 pagesBlood Glucose MonitoringAman ChaudharyNo ratings yet
- Mental StatusDocument6 pagesMental StatusIgor Oliveira100% (1)
- Scientific and Ethical Issues in The Use of Placebo Controls in Clinical TrialsDocument20 pagesScientific and Ethical Issues in The Use of Placebo Controls in Clinical TrialsNicusor OnaciuNo ratings yet
- Infection Control Practice On Vital Signs Equipment: A Survey Among Senior Nursing Students in Iloilo City, PhilippinesDocument7 pagesInfection Control Practice On Vital Signs Equipment: A Survey Among Senior Nursing Students in Iloilo City, PhilippinesRyan Michael OducadoNo ratings yet
- Attributable Fractions (As11) : Course: PG Diploma/ MSC EpidemiologyDocument37 pagesAttributable Fractions (As11) : Course: PG Diploma/ MSC EpidemiologyLakshmi SethNo ratings yet
- KUsta PDFDocument29 pagesKUsta PDFTokekKompieNo ratings yet
- Mallory Brearey-Resume 2021 1Document2 pagesMallory Brearey-Resume 2021 1api-507675724No ratings yet