You might also like
- Marketing Implant Dentistry: Attract and Influence Patients to Accept Your Dental Implant Treatment PlanFrom EverandMarketing Implant Dentistry: Attract and Influence Patients to Accept Your Dental Implant Treatment PlanNo ratings yet
- RCDSO Guidelines Implant DentistryDocument16 pagesRCDSO Guidelines Implant DentistrydoctorlupuNo ratings yet
- Fixed Prosthodontics Clinic Manual 2015-2016Document73 pagesFixed Prosthodontics Clinic Manual 2015-2016wendyjemmy8gmailcomNo ratings yet
- Professional Competencies of The Newly Qualified DentistDocument15 pagesProfessional Competencies of The Newly Qualified DentistDiana Stephen BernardNo ratings yet
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- Introduction To OcclusionDocument56 pagesIntroduction To OcclusionSuvasish SuvasishNo ratings yet
- Dentaltown 2018marchDocument113 pagesDentaltown 2018marchDanutz BalanNo ratings yet
- Swift Series Clinical Governance Book Edition 1Document69 pagesSwift Series Clinical Governance Book Edition 1Lily Hariri100% (1)
- PLPF PDFDocument88 pagesPLPF PDFmaxNo ratings yet
- 5 Steps To A Successful Dental PracticeDocument22 pages5 Steps To A Successful Dental PracticeVasile FlorinNo ratings yet
- Pre Treatment Assesment of ImplantDocument19 pagesPre Treatment Assesment of Implantdrgayen6042No ratings yet
- AOCMF OfflineApplicationDocument2 pagesAOCMF OfflineApplicationArif Tri Prasetyo HarunNo ratings yet
- Common Mistakes in Clinical Dental PracticeDocument80 pagesCommon Mistakes in Clinical Dental PracticeRohit ShahNo ratings yet
- #2 - PEDO Final - Record Keeping & Treatment PlanningDocument24 pages#2 - PEDO Final - Record Keeping & Treatment PlanningomeerulrafieNo ratings yet
- MagnificationDocument52 pagesMagnificationSiva KumarNo ratings yet
- Optimization of Emergence Profile of Implant ProstDocument8 pagesOptimization of Emergence Profile of Implant ProstAya Ibrahim YassinNo ratings yet
- Bedrossian Treatment Planning The Maxilla PDFDocument11 pagesBedrossian Treatment Planning The Maxilla PDFSitiKhadijahNo ratings yet
- An Ounce of Prevention Is Worth A Pound of Cure: Ergonomics in Dental PracticeDocument6 pagesAn Ounce of Prevention Is Worth A Pound of Cure: Ergonomics in Dental Practicetri wahyuniNo ratings yet
- MGE Case Acceptance Ebook 2018 PDFDocument22 pagesMGE Case Acceptance Ebook 2018 PDFMavisNo ratings yet
- ITI Decision Tree Immediate PlacementDocument1 pageITI Decision Tree Immediate Placementxiaoxin zhangNo ratings yet
- Erosion Abrasion Attrition and Abfrcation1Erosion Abrasion Attrition and Abfrcation1Document82 pagesErosion Abrasion Attrition and Abfrcation1Erosion Abrasion Attrition and Abfrcation1Madalina A DobreNo ratings yet
- AO Trauma CMFDocument9 pagesAO Trauma CMFAldo AguilarNo ratings yet
- Working Length DeterminationDocument97 pagesWorking Length Determinationrolly_jatinNo ratings yet
- Managing The Unstable CDDocument8 pagesManaging The Unstable CDNajeeb UllahNo ratings yet
- Volumetric Shrinkage and Film THDocument8 pagesVolumetric Shrinkage and Film THcalebleon101113No ratings yet
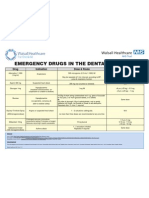
- Emergency Drugs Poster - Layout 1 in Dental PracticeDocument1 pageEmergency Drugs Poster - Layout 1 in Dental PracticeFady AtefNo ratings yet
- Caries Detection and Diagnosis Sealants and Management of The Possibly Carious Fissure PDFDocument7 pagesCaries Detection and Diagnosis Sealants and Management of The Possibly Carious Fissure PDFGen LCNo ratings yet
- Wang 2021 Imagenologíaen CBMFDocument21 pagesWang 2021 Imagenologíaen CBMFRocio CacñahuarayNo ratings yet
- DR - Hassan Dental Auxillary-3 (Muhadharaty)Document33 pagesDR - Hassan Dental Auxillary-3 (Muhadharaty)علي موسى مهديNo ratings yet
- ACP Digital Dentistry CurriculumDocument120 pagesACP Digital Dentistry Curriculumد.أحمد محمدNo ratings yet
- Implant Patient Surgery Information and Consent FormDocument5 pagesImplant Patient Surgery Information and Consent FormtinkfayeNo ratings yet
- Oxford Assess and Progress Clinical DentistryDocument361 pagesOxford Assess and Progress Clinical Dentistrysmustafa.officeNo ratings yet
- 10867-0 Neoss Anatomical Healing Abutment Manual Hi Res 2009-05-19Document4 pages10867-0 Neoss Anatomical Healing Abutment Manual Hi Res 2009-05-19Nate TaylorNo ratings yet
- After Extraction InstructionDocument4 pagesAfter Extraction Instructionmelly andrieNo ratings yet
- 2015 @dentallib Jonathan B LevineDocument298 pages2015 @dentallib Jonathan B LevineM.A.Preto100% (1)
- IMPLANTOLOGI Compressed Compressed (1) - MinDocument122 pagesIMPLANTOLOGI Compressed Compressed (1) - MinNayafilahNo ratings yet
- ASDA NewsletterDocument16 pagesASDA NewsletterThomas LaNo ratings yet
- Clin DSDDocument5 pagesClin DSDAlfred OrozcoNo ratings yet
- Aesthetic Evolution - 7 Lessons of Indirect RestorationDocument10 pagesAesthetic Evolution - 7 Lessons of Indirect RestorationAndreea StaicuNo ratings yet
- A A D W - Up: N Dvanced Iagnostic AxDocument4 pagesA A D W - Up: N Dvanced Iagnostic AxjoephinNo ratings yet
- En PeriimplantitaDocument312 pagesEn PeriimplantitaDan Țăruș100% (1)
- Implant Consent Form1Document2 pagesImplant Consent Form1Jitender ReddyNo ratings yet
- Dental 22Document18 pagesDental 22SurabiNo ratings yet
- Dentistry: Primary Dental Care Services in England and WalesDocument72 pagesDentistry: Primary Dental Care Services in England and WalesAyman BafaQeehNo ratings yet
- Implant Course.Document76 pagesImplant Course.mustafaNo ratings yet
- The Official Journal of The Academy of Laser DentistryDocument72 pagesThe Official Journal of The Academy of Laser DentistrySalim MalikNo ratings yet
- EthicsDocument54 pagesEthicsMehek BatraNo ratings yet
- Use of Implants in The Pterygoid Region For Prosthodontic TreatmentDocument4 pagesUse of Implants in The Pterygoid Region For Prosthodontic TreatmentSidhartha KumarNo ratings yet
- Controversiesin Anesthesiafororaland Maxillofacialsurgery: Brett J. King,, Adam LevineDocument9 pagesControversiesin Anesthesiafororaland Maxillofacialsurgery: Brett J. King,, Adam LevineAB MISHRANo ratings yet
- Papper PeriodDocument12 pagesPapper PeriodLoretoReyesMoralesNo ratings yet
- Risk FactorsDocument174 pagesRisk FactorsdevikaNo ratings yet
- 2 Nonsurgical Periodontal Therapy - Pocket DentistryDocument14 pages2 Nonsurgical Periodontal Therapy - Pocket DentistryRizki OktavianiNo ratings yet
- Pulp Therapy For Primary and Immature Permanent TeethDocument11 pagesPulp Therapy For Primary and Immature Permanent TeethPrabhjot KaurNo ratings yet
- Multimedia PDFDocument16 pagesMultimedia PDFadamNo ratings yet
- Implant ResearchDocument8 pagesImplant ResearchFBI LUC1FeRNo ratings yet
- Existing Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDocument47 pagesExisting Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDaniel WangNo ratings yet
- Immediate Implant Placement PDFDocument11 pagesImmediate Implant Placement PDFFerdinan PasaribuNo ratings yet
- Oral and Maxillofacial Surgery Clinics of North America Office Based Anesthesia 45 57Document13 pagesOral and Maxillofacial Surgery Clinics of North America Office Based Anesthesia 45 57Max FaxNo ratings yet
- PEAK Botulinum Toxin and Dentistry PDFDocument4 pagesPEAK Botulinum Toxin and Dentistry PDFl4j0b9No ratings yet
- Laboratory Catalog PDFDocument48 pagesLaboratory Catalog PDFl4j0b9No ratings yet
- Oda HDocument82 pagesOda Hl4j0b9No ratings yet
- PEAK Botulinum Toxin and Dentistry PDFDocument4 pagesPEAK Botulinum Toxin and Dentistry PDFl4j0b9No ratings yet
- RCDSO Standard of Practice Dental CT ScannersDocument8 pagesRCDSO Standard of Practice Dental CT Scannersl4j0b9No ratings yet
- Funny StoriesDocument5 pagesFunny Storiesamin jamalNo ratings yet
- Neuroscience: Science of The Brain in PolishDocument72 pagesNeuroscience: Science of The Brain in PolishInternational Brain Research Organization100% (1)
- Aetna Insurance DecisionDocument13 pagesAetna Insurance DecisionJeffStelling1No ratings yet
- PAS HAndbookDocument375 pagesPAS HAndbookJheanell JamesNo ratings yet
- PlacentaDocument21 pagesPlacentaAttiqaQureshiNo ratings yet
- English - Modern vs. Traditional MedicineDocument11 pagesEnglish - Modern vs. Traditional MedicineJoao AlfandegaNo ratings yet
- Aceclofenac Vs Diclofenac On Hexosamine LevelsDocument11 pagesAceclofenac Vs Diclofenac On Hexosamine LevelsMartin MoranNo ratings yet
- Retroauricular Abscess Case ReportDocument2 pagesRetroauricular Abscess Case ReportYuna WidjajaNo ratings yet
- Clinical Abstract FormDocument1 pageClinical Abstract FormHihiNo ratings yet
- Update Stock PT KMD 14-6Document46 pagesUpdate Stock PT KMD 14-6rio1995No ratings yet
- KARDEX Case 3Document3 pagesKARDEX Case 3Juviely PremacioNo ratings yet
- Direct Pulp Capping in Primary Molars: Report of Two CasesDocument3 pagesDirect Pulp Capping in Primary Molars: Report of Two Casesemie sitorusNo ratings yet
- BC CancerDocument42 pagesBC CancerIsal SparrowNo ratings yet
- Marinedrugs 17 00636 PDFDocument24 pagesMarinedrugs 17 00636 PDFNindah IkaNo ratings yet
- German Marine Agencies, Inc., Et Al. Petitioners, vs. Teodolah R. Caro, in Behalf of Her Husband Eduardo v. Caro, Respondent.Document5 pagesGerman Marine Agencies, Inc., Et Al. Petitioners, vs. Teodolah R. Caro, in Behalf of Her Husband Eduardo v. Caro, Respondent.Francis Coronel Jr.No ratings yet
- Pathophysiology of TetanusDocument2 pagesPathophysiology of TetanusAnitha SuprionoNo ratings yet
- Article 007Document6 pagesArticle 007Dyah Putri Ayu DinastyarNo ratings yet
- Tryptophan Supplement For SleepDocument35 pagesTryptophan Supplement For SleepZie Dak BlurNo ratings yet
- WC500059147 PDFDocument140 pagesWC500059147 PDFAnaStankovićNo ratings yet
- Ge Cumulative Rates ResortedDocument81 pagesGe Cumulative Rates ResortedfishyfredNo ratings yet
- An Approach To The Management of Hyperbilirubinemia in The Preterm Infant Less Than 35 Weeks of GestationDocument5 pagesAn Approach To The Management of Hyperbilirubinemia in The Preterm Infant Less Than 35 Weeks of Gestationberthad33No ratings yet
- Biochemistry Reagents - ITA Kits - Promotional Tool 27th - August-2019-2Document23 pagesBiochemistry Reagents - ITA Kits - Promotional Tool 27th - August-2019-2Ajay DataniyaNo ratings yet
- 1999 CQfirstphaseallotments PDFDocument73 pages1999 CQfirstphaseallotments PDFISMAIL KHANNo ratings yet
- Alprazolam Effect On ThyroidDocument7 pagesAlprazolam Effect On ThyroidswatiNo ratings yet
- Terumo PenpolDocument6 pagesTerumo PenpolJhony SebanNo ratings yet
- SDocument34 pagesSRam Kumar YadavNo ratings yet
- Obsgyn BooksDocument4 pagesObsgyn BooksYulian NuswantoroNo ratings yet
- DVand Video ArthroscopesDocument2 pagesDVand Video Arthroscopesapi-19808945No ratings yet
- MCQs 1Document10 pagesMCQs 1Mostafa MahmoudNo ratings yet
- SMART Nano Probes For Targeting Diseased Sites. Dr. Rao PapineniDocument1 pageSMART Nano Probes For Targeting Diseased Sites. Dr. Rao PapineniPapineni LabsNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (30)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (5)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- Empath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainFrom EverandEmpath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainRating: 4 out of 5 stars4/5 (95)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (61)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (59)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (45)