You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- 1brisbane Final ReportDocument49 pages1brisbane Final ReportAustralian Human Rights100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Audit Observations and Recommendations on Gender and Development FundsDocument43 pagesAudit Observations and Recommendations on Gender and Development FundsJonson PalmaresNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Leadership Training - Freedom ScaleDocument3 pagesLeadership Training - Freedom Scalefractalbops138No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Punjab Health FoundationDocument29 pagesPunjab Health FoundationAhsan 11No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- PFF002 EmployersDataForm V06Document2 pagesPFF002 EmployersDataForm V06hitme bensiNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Integrated Child Development Scheme (ICDS)Document30 pagesIntegrated Child Development Scheme (ICDS)Geeta KumariNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Employment Opportunity Assistant CoordinatorDocument2 pagesEmployment Opportunity Assistant CoordinatorKagitaMikamNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Admission Criteria For MBBSDocument7 pagesAdmission Criteria For MBBSGautam AggarwalNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Medical EduDocument94 pagesMedical EdudeshpandebjNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
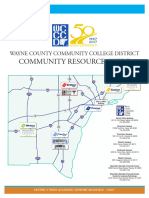
- Wayne County Community Resource GuideDocument14 pagesWayne County Community Resource GuideWXYZ-TV Channel 7 DetroitNo ratings yet
- A Case Study On Vellore Citizens Welfare Forum Vs Union of India With Special Reference To Polluters Pay Principle J.Sabitha J.Tamil SelviDocument10 pagesA Case Study On Vellore Citizens Welfare Forum Vs Union of India With Special Reference To Polluters Pay Principle J.Sabitha J.Tamil SelviJ Sab IthaNo ratings yet
- 30 Hour Construction Final Exam Answer KeyDocument74 pages30 Hour Construction Final Exam Answer KeyJames Warden78% (23)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Application Form IberoDocument2 pagesApplication Form IberodaneshnedaieNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Economics 1st Lesson PDFDocument1 pageEconomics 1st Lesson PDFSandy SaddlerNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Sosialisasi E-Report IKP RS Eksternal - 2021Document32 pagesSosialisasi E-Report IKP RS Eksternal - 2021Putri Arum PermatasariNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Professional Responsibility and AccountabilityDocument5 pagesProfessional Responsibility and Accountabilityjasdeepkaurnagra100% (2)
- Refusal To Treat A PatientDocument4 pagesRefusal To Treat A Patientzwecker4458No ratings yet
- Adv PDocument3 pagesAdv Pamiable_sudipNo ratings yet
- TranscriptDocument6 pagesTranscriptjohn doeNo ratings yet
- Applicant Biographic Details and Travel Date: Official Use OnlyDocument11 pagesApplicant Biographic Details and Travel Date: Official Use OnlyprashanthNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- FORMUL 01796 Lipstick-FormulationDocument2 pagesFORMUL 01796 Lipstick-FormulationSham Saja100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Ga 16Document6 pagesGa 16somu645No ratings yet
- BS8313Document54 pagesBS8313Donald HamiltonNo ratings yet
- EC325 Week 7 Problem SetDocument2 pagesEC325 Week 7 Problem SetViraj MehtaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Full David Brock Confidential Memo On Fighting Trump Gray OCRedDocument49 pagesFull David Brock Confidential Memo On Fighting Trump Gray OCRedstarina2No ratings yet
- Drugs & Cosmetics ActDocument70 pagesDrugs & Cosmetics ActAnonymous ibmeej9No ratings yet
- IssueMarch2017 April2017 PDFDocument20 pagesIssueMarch2017 April2017 PDFDavid ThomasNo ratings yet
- How Should QuickMedx GrowDocument1 pageHow Should QuickMedx Growg14025No ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Local Government Code of The PhilippinesDocument6 pagesThe Local Government Code of The PhilippinesAngeliqueNo ratings yet
- Uniform System Of Accounts For The Lodging Industry | Major ChangesDocument8 pagesUniform System Of Accounts For The Lodging Industry | Major ChangestodowedeNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)