You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Reiki Book PDFDocument108 pagesReiki Book PDFGurpreet Singh Sohal100% (1)
- Coping With Loss, Grief, DeathDocument23 pagesCoping With Loss, Grief, Deathsoumya sathesh100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- EPISCLERITIS & ScleritisDocument14 pagesEPISCLERITIS & ScleritisChikita Artia SariNo ratings yet
- Expectorant and Demulcent HerbsDocument3 pagesExpectorant and Demulcent HerbsqueencelNo ratings yet
- Agbo Yoruba 1Document37 pagesAgbo Yoruba 1Nass Minallahi Adekunle93% (69)
- Veterinary Pharmacology and Toxicology MCQsDocument18 pagesVeterinary Pharmacology and Toxicology MCQsSunil97% (63)
- Aub Updated-1 PDFDocument87 pagesAub Updated-1 PDFEvelyn Pamela Espinoza Morales100% (2)
- Guidelines Emergency Medicine Pharmacist ServicesDocument15 pagesGuidelines Emergency Medicine Pharmacist ServicesMárcio BatistaNo ratings yet
- ANNEXURE-5 Material Safety Data SheetDocument11 pagesANNEXURE-5 Material Safety Data SheetSuraj KumarNo ratings yet
- Dilated CardiomyopathyDocument13 pagesDilated CardiomyopathyPrincysuzine PintoNo ratings yet
- Chinese Food TherapyDocument5 pagesChinese Food TherapyDoktormin106No ratings yet
- The Chemistry of Beef FlavorDocument16 pagesThe Chemistry of Beef FlavorNada Hren100% (1)
- Orbital Trauma NCP and Drug StudyDocument5 pagesOrbital Trauma NCP and Drug StudyDersly LaneNo ratings yet
- Meloxicam For DogsDocument2 pagesMeloxicam For DogsNada HrenNo ratings yet
- Flavours From AminoacidsDocument31 pagesFlavours From AminoacidsNada HrenNo ratings yet
- Maxflow CaDocument10 pagesMaxflow CaNada HrenNo ratings yet
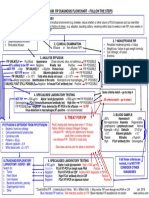
- Follow The Steps: 1. History 2. ? Effusive FipDocument1 pageFollow The Steps: 1. History 2. ? Effusive FipNada HrenNo ratings yet
- Dickinson 2020 Antiviral Treatment Using The Adeno PDFDocument7 pagesDickinson 2020 Antiviral Treatment Using The Adeno PDFNada HrenNo ratings yet
- Using Feline Recombinant Omega InterferonDocument1 pageUsing Feline Recombinant Omega InterferonNada HrenNo ratings yet
- Viruses: Clinical Aspects of Feline Retroviruses: A ReviewDocument27 pagesViruses: Clinical Aspects of Feline Retroviruses: A ReviewNada HrenNo ratings yet
- Introduction To DistillationDocument39 pagesIntroduction To DistillationNada HrenNo ratings yet
- Love Spells That Work Fast with money back guaranteed results in USA, Australia, Canada, UK, UAE, Norway, Finland, Ireland, Iceland, Namibia, Kenya, Botswana, Florida, Wales, Denmark, Sweden+27733947689Document4 pagesLove Spells That Work Fast with money back guaranteed results in USA, Australia, Canada, UK, UAE, Norway, Finland, Ireland, Iceland, Namibia, Kenya, Botswana, Florida, Wales, Denmark, Sweden+27733947689prof talik0% (1)
- Toxicidd de Anestesicos Locales1Document6 pagesToxicidd de Anestesicos Locales1Sintia Andrea Peñaloza FernándezNo ratings yet
- Corneal Sensitivity and Ocular Surface Changes Following Preserved Amniotic Membrane Transplantation For Nonhealing Corneal UlcersDocument10 pagesCorneal Sensitivity and Ocular Surface Changes Following Preserved Amniotic Membrane Transplantation For Nonhealing Corneal UlcersDitha FadhilaNo ratings yet
- Endogenous Intoxication in SurgeryDocument5 pagesEndogenous Intoxication in SurgeryJonah Seeni100% (1)
- Cues/ Evidences Nursing Diagnosi S Scientific Basis Goals and Outcome Criteria Nursing Actions and Nursing Orders Rationale of Nursing Actions EvaluationDocument5 pagesCues/ Evidences Nursing Diagnosi S Scientific Basis Goals and Outcome Criteria Nursing Actions and Nursing Orders Rationale of Nursing Actions EvaluationCharlene Serino JavierNo ratings yet
- Hyperemesis Gravidarum Hyperemesis Gravidarum: Brief ReviewDocument8 pagesHyperemesis Gravidarum Hyperemesis Gravidarum: Brief ReviewMISSLADYTIGNERNo ratings yet
- Efficacy of Homeopathic Medicines in Ren PDFDocument15 pagesEfficacy of Homeopathic Medicines in Ren PDFJoana R. SilvaNo ratings yet
- Maklumat Struktur Pengajian Bachelor of Medical Science (With Credit Exemption)Document2 pagesMaklumat Struktur Pengajian Bachelor of Medical Science (With Credit Exemption)Noraini Mohammad YusufNo ratings yet
- S03 - FPSC Mayur Vihar Extension Shop No-07, Atlantic Plaza, Plot No-1 Samachar Market, Mayur Vihar Phase-1-Ext Mobil No:9811051975Document2 pagesS03 - FPSC Mayur Vihar Extension Shop No-07, Atlantic Plaza, Plot No-1 Samachar Market, Mayur Vihar Phase-1-Ext Mobil No:9811051975Mriganabh ChoudhuryNo ratings yet
- 001000000000085025Document1 page001000000000085025Irfan Ullah KhanNo ratings yet
- Names of Professions in HospitalDocument23 pagesNames of Professions in HospitalnadyaNo ratings yet
- Destive System: What Is Digestion?Document2 pagesDestive System: What Is Digestion?Pepy PeachNo ratings yet
- Resume Lismari Reyes MunozDocument2 pagesResume Lismari Reyes Munozapi-253469228No ratings yet
- Analgesic Efficacy of Erector Spinae Plane BlocksDocument7 pagesAnalgesic Efficacy of Erector Spinae Plane BlocksAlejandra SanchezNo ratings yet
- ERCP-related Adverse Events: European Society of Gastrointestinal Endoscopy (ESGE) GuidelineDocument24 pagesERCP-related Adverse Events: European Society of Gastrointestinal Endoscopy (ESGE) GuidelineFarid RakhmanNo ratings yet
- SURGERY WARD-WPS OfficeDocument4 pagesSURGERY WARD-WPS OfficeMary Claire MasoNo ratings yet
- Unoccupied Bed: ProcedureDocument7 pagesUnoccupied Bed: ProcedurechinztrolNo ratings yet
- U V - 1 C-Avz-O-Qtzb: Question Paper Specific InstructionsDocument5 pagesU V - 1 C-Avz-O-Qtzb: Question Paper Specific InstructionsBrij Nandan PrasadNo ratings yet