You might also like
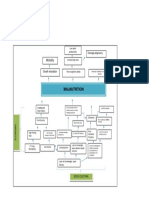
- Problem Tree Analysis MalnutritionDocument1 pageProblem Tree Analysis MalnutritionMho Dsb50% (6)
- PediatricsDocument98 pagesPediatricsNicholas Field100% (1)
- CADASIL: Main Clinical Features and Natural History by Hugues ChabriatDocument33 pagesCADASIL: Main Clinical Features and Natural History by Hugues ChabriatFondation Singer-PolignacNo ratings yet
- Wanda POS Administrator's GuideDocument65 pagesWanda POS Administrator's GuideVictor PorrasNo ratings yet
- Cyclophosphamide vs Mycophenylate mofetil for lupus nephritisDocument39 pagesCyclophosphamide vs Mycophenylate mofetil for lupus nephritisTalal Ali KhanNo ratings yet
- Cazuri CliniceDocument32 pagesCazuri CliniceHeba VerebceanNo ratings yet
- Tuberculous MeningitisDocument34 pagesTuberculous MeningitisSubchanPrasetyoNo ratings yet
- Hepatitis C Primer For HIV Care ProvidersDocument26 pagesHepatitis C Primer For HIV Care ProvidersSaad MotawéaNo ratings yet
- Male Infertility: G. Wirya K. DuarsaDocument46 pagesMale Infertility: G. Wirya K. DuarsaJuli FionaNo ratings yet
- Emmanuel Rivers SlidesDocument91 pagesEmmanuel Rivers SlidescarlodapNo ratings yet
- CML PresentationDocument55 pagesCML PresentationИван НегарэNo ratings yet
- Golden NumbersDocument89 pagesGolden NumbersjoobazhieNo ratings yet
- Adpkd CursDocument56 pagesAdpkd Cursplaiul mioriticNo ratings yet
- Early PrediabetesDocument4 pagesEarly Prediabetesvicky ortizNo ratings yet
- Plasma Homocysteine, Fasting Insulin, and Serum Androgens As A Function of Sonographic Ovarian FeaturesDocument20 pagesPlasma Homocysteine, Fasting Insulin, and Serum Androgens As A Function of Sonographic Ovarian FeaturesDenisNo ratings yet
- Am J Surg 2004 p463Document4 pagesAm J Surg 2004 p463olivia magdalenaNo ratings yet
- Tuberculous Meningitis Diagnosis, Treatment and Impact of HIVDocument34 pagesTuberculous Meningitis Diagnosis, Treatment and Impact of HIVLuvi PujiNo ratings yet
- Characterization of Classical and Neoclassical Fabry Disease - A Multicenter StudyDocument11 pagesCharacterization of Classical and Neoclassical Fabry Disease - A Multicenter StudyUlisesNo ratings yet
- Catastrophic Antiphospholipid Syndrome: Triggers, Presentation, Diagnosis and ManagementDocument24 pagesCatastrophic Antiphospholipid Syndrome: Triggers, Presentation, Diagnosis and ManagementJiayu YangNo ratings yet
- Pediatric Acute Renal Failure: CRRT/Dialysis Outcome StudiesDocument25 pagesPediatric Acute Renal Failure: CRRT/Dialysis Outcome StudiesCF PonceNo ratings yet
- 2019 Glomerulonefritis Pos-Inf Pedi Clin NADocument14 pages2019 Glomerulonefritis Pos-Inf Pedi Clin NA0511821012 KATHERIN YULEIMA CAMACHO MARIN ESTUDIANTE ACTIVONo ratings yet
- Electrocardiographic Predictors of Incident Atrial Fibrillation - DavidDocument6 pagesElectrocardiographic Predictors of Incident Atrial Fibrillation - DavidDavid Jimmy Kurniawan RejosaputroNo ratings yet
- Association of Serum Uric Acid and Cardiovascular Disease in Healthy AdultsDocument7 pagesAssociation of Serum Uric Acid and Cardiovascular Disease in Healthy Adultsfeti_08No ratings yet
- Missed Opportunities An Observational Study of Vital SignsDocument6 pagesMissed Opportunities An Observational Study of Vital SignsZeera MohamadNo ratings yet
- NC Rara HemaDocument18 pagesNC Rara HemaDodi DiNo ratings yet
- CKDDocument48 pagesCKDJuniorNo ratings yet
- Jurnal 4Document11 pagesJurnal 4Kholifatu UlfaNo ratings yet
- Anesthetic Considerations in Obstetric EmergenciesDocument45 pagesAnesthetic Considerations in Obstetric EmergenciesPaul HerreraNo ratings yet
- Oncology For The Internist Cancer Screening: Devapiran Jaishankar Associate Professor EtsuDocument64 pagesOncology For The Internist Cancer Screening: Devapiran Jaishankar Associate Professor EtsuSalman Muazzam MuddassirNo ratings yet
- 5 - Colecistitis 2017Document23 pages5 - Colecistitis 2017JaimeNo ratings yet
- A 19 Year Old With Fever, Rash, and Conjunctivitis: A Connection With The HeartDocument3 pagesA 19 Year Old With Fever, Rash, and Conjunctivitis: A Connection With The HeartLeberina TunjNo ratings yet
- Management of Breast CancerDocument53 pagesManagement of Breast CancerGaoudam NatarajanNo ratings yet
- Oct'23Document23 pagesOct'23saieefzaman71No ratings yet
- Case FormatDocument12 pagesCase FormatMaria VisitacionNo ratings yet
- Peripheral Arterial DiseaseDocument161 pagesPeripheral Arterial Diseasec406400No ratings yet
- Microalbuminuria Predicts Mortality in ElderlyDocument4 pagesMicroalbuminuria Predicts Mortality in Elderlyilma_ilemNo ratings yet
- Clinical Study: Development of Dengue Infection Severity ScoreDocument6 pagesClinical Study: Development of Dengue Infection Severity ScoreValencius SunandarNo ratings yet
- Gastroenterology PT MRCP I 2019 2nd Edition PDF HXP DR NotesDocument1,142 pagesGastroenterology PT MRCP I 2019 2nd Edition PDF HXP DR NotesRami NaousNo ratings yet
- 2100 7840 1 PBDocument7 pages2100 7840 1 PB蘇柏霖No ratings yet
- Diagnostic Yield of Cytopathology in Evaluating Pericardial Effusions: Clinicopathologic Analysis of 419 SpecimensDocument10 pagesDiagnostic Yield of Cytopathology in Evaluating Pericardial Effusions: Clinicopathologic Analysis of 419 SpecimensAnca CucuNo ratings yet
- Lecture SlidesDocument66 pagesLecture SlidesAymen JamalNo ratings yet
- Technologies Designed To Help Improve Patients OutcomeDocument53 pagesTechnologies Designed To Help Improve Patients OutcomeHarby Ongbay AbellanosaNo ratings yet
- Acute Pancreatitis Guide: Causes, Symptoms, Diagnosis and TreatmentDocument34 pagesAcute Pancreatitis Guide: Causes, Symptoms, Diagnosis and TreatmentDrscottmccallNo ratings yet
- Infectious Diseases: Smart Study Guide for Medical Students, Residents, and Clinical ProvidersFrom EverandInfectious Diseases: Smart Study Guide for Medical Students, Residents, and Clinical ProvidersNo ratings yet
- Etiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisDocument8 pagesEtiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisakhmadNo ratings yet
- HIV Neurology: Graeme MeintjesDocument75 pagesHIV Neurology: Graeme MeintjesPrincess MiraNo ratings yet
- Ovarian Sertoli-Leydig Cell Tumors Epidemiological Clinical and Prognostic FactorsDocument9 pagesOvarian Sertoli-Leydig Cell Tumors Epidemiological Clinical and Prognostic FactorsJosé LuisNo ratings yet
- Nexavar in Patients With Renal Cell Carcinoma: Naomi B. Haas October 4, 2007Document58 pagesNexavar in Patients With Renal Cell Carcinoma: Naomi B. Haas October 4, 2007Jenna AbuanNo ratings yet
- Angina Pectoris and Atherosclerotic Risk Factors in The MultisiteDocument8 pagesAngina Pectoris and Atherosclerotic Risk Factors in The Multisiteger4ld1nNo ratings yet
- Clinical characteristics and outcomes of hepatitis C patients throughout treatmentDocument3 pagesClinical characteristics and outcomes of hepatitis C patients throughout treatmentIslam NasrNo ratings yet
- Steroid-Responsive Encephalopathy Associated With Autoimmune ThyroiditisDocument6 pagesSteroid-Responsive Encephalopathy Associated With Autoimmune ThyroiditisRafael MartinsNo ratings yet
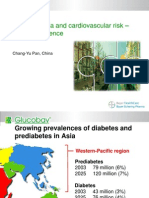
- Asia - Pan - Dysglycaemia and Cardiovascular Risk Û Asian ExperienceDocument18 pagesAsia - Pan - Dysglycaemia and Cardiovascular Risk Û Asian ExperienceputrakartonoNo ratings yet
- 7.13.09 Dooley Lupus NephritisDocument39 pages7.13.09 Dooley Lupus NephritisbogdansoroNo ratings yet
- Clinico-Etiological Spectrum of Pancytopenia in Hospitalized ChildrenDocument4 pagesClinico-Etiological Spectrum of Pancytopenia in Hospitalized ChildrenNurul Huda KowitaNo ratings yet
- Detecting Ascites and Performing Safe ParacentesisDocument10 pagesDetecting Ascites and Performing Safe ParacentesisOscar Diaz PeraltaNo ratings yet
- ASH Hematology Review Series - Hodgkin Lymphoma - HerreraDocument69 pagesASH Hematology Review Series - Hodgkin Lymphoma - HerreraИван НегарэNo ratings yet
- 4 Current Management of Esophageal Atresia and Tracheoesophageal FistulaDocument38 pages4 Current Management of Esophageal Atresia and Tracheoesophageal FistulaTurabayo Jean LéonardNo ratings yet
- Cirrosis Biliar Primaria: Experiencia de Trece Años en Dos Centros de ReferenciaDocument6 pagesCirrosis Biliar Primaria: Experiencia de Trece Años en Dos Centros de ReferenciaEdgar UribeNo ratings yet
- Acquired Disorders SpermatogenesisDocument36 pagesAcquired Disorders SpermatogenesisjlasaNo ratings yet
- Enteral Nutrition Therapy For The Surgical PatientDocument52 pagesEnteral Nutrition Therapy For The Surgical PatientelenNo ratings yet
- Hodgkin PresentationDocument55 pagesHodgkin PresentationThe Ray Medicster100% (1)
- Liver Disease: A Clinical CasebookFrom EverandLiver Disease: A Clinical CasebookStanley Martin CohenNo ratings yet
- DinithDocument102 pagesDinithVishmi amashaNo ratings yet
- SMRP SAMPLE Guide To The Maintenance and ReliabiliDocument17 pagesSMRP SAMPLE Guide To The Maintenance and ReliabiliSaul sanchez MantillaNo ratings yet
- List of Intel Core I3 MicroprocessorsDocument3 pagesList of Intel Core I3 MicroprocessorsKing 79100% (1)
- PHD Thesis Environmental LawDocument5 pagesPHD Thesis Environmental LawPaySomeoneToWriteYourPaperPittsburgh100% (2)
- TM55 1520 242 MTFDocument192 pagesTM55 1520 242 MTFJakub Kostka100% (1)
- Agoraphobia - Simmel and Kracauer - Anthony VidlerDocument16 pagesAgoraphobia - Simmel and Kracauer - Anthony VidlerArthur BuenoNo ratings yet
- Leiter-3 Appendix D New 2014Document6 pagesLeiter-3 Appendix D New 2014Didenko MarinaNo ratings yet
- Kerala University of Health Sciences Faculty of Dentistry BDS Course Regulations and Syllabus 2010Document125 pagesKerala University of Health Sciences Faculty of Dentistry BDS Course Regulations and Syllabus 2010Shyam KrishnanNo ratings yet
- Soal B Inggris Uas KLS X OllaDocument25 pagesSoal B Inggris Uas KLS X OllaRidwan, S.Pd.,M.SiNo ratings yet
- Moon Landing ConspiracyDocument17 pagesMoon Landing ConspiracyElianeSalamNo ratings yet
- Kalayaan Island GroupDocument17 pagesKalayaan Island Group202030166No ratings yet
- Ponnu ThomasDocument155 pagesPonnu ThomasWinston KennethNo ratings yet
- Lecture 2 2014 Random Errors in Chemical AnalysisDocument24 pagesLecture 2 2014 Random Errors in Chemical AnalysisRobert EdwardsNo ratings yet
- Cyber Security Module 1Document4 pagesCyber Security Module 1silentnightNo ratings yet
- Civ Pro I - 2011 TahaDocument27 pagesCiv Pro I - 2011 TahaACDCNo ratings yet
- MICEDocument37 pagesMICECeleste Torino DigalNo ratings yet
- NATO Intelligence Exploitation of The InternetDocument104 pagesNATO Intelligence Exploitation of The Internetmauro.pennacchietti100% (1)
- 10 - Bus 105 and 107-1Document400 pages10 - Bus 105 and 107-1Alao LateefNo ratings yet
- Organic ReactionsDocument73 pagesOrganic ReactionsKrishnaah Doraj100% (1)
- Philippine citizenship law allows dual citizenshipDocument9 pagesPhilippine citizenship law allows dual citizenshipriaheartsNo ratings yet
- The Nazi Master PlanDocument28 pagesThe Nazi Master PlanFolad109No ratings yet
- Mutagenic Effects of Sodium Azide On The Quality of Maize SeedsDocument7 pagesMutagenic Effects of Sodium Azide On The Quality of Maize SeedsKanhiya MahourNo ratings yet
- How To... Train Managers As Coaches: Shaun LincolnDocument2 pagesHow To... Train Managers As Coaches: Shaun LincolnBenny fernandesNo ratings yet
- Difference Between Society and CommunityDocument2 pagesDifference Between Society and CommunityashnajananNo ratings yet
- Esophageal Carcinoma: Preceptor: Dr. Ratesh KhillanDocument37 pagesEsophageal Carcinoma: Preceptor: Dr. Ratesh KhillanVarun VarnNo ratings yet
- SalmonellaDocument2 pagesSalmonellaAlfarizi Julistyo S.No ratings yet
- 5 All India Mobile Database SampleDocument15 pages5 All India Mobile Database Sampleali khan Saifi100% (1)
- Customer Preferences For Restaurant Technology InnovationsDocument22 pagesCustomer Preferences For Restaurant Technology InnovationsDeepankar SinghNo ratings yet