DOI: 10.5958/j.2319-5886.3.2.
095
International Journal of Medical Research & Health Sciences
www.ijmrhs.com Volume 3 Issue 2 (April - Jun) Coden: IJMRHS th Received: 30 Dec 2013 Revised: 25th Jan 2014
Case report
Copyright @2014 ISSN: 2319-5886 Accepted: 30th Jan 2014
FETAL DIPROSOPUS (DOUBLE FACE): A CASE REPORT *Onankpa BO1, Ukwu E2, Singh S2, Adoke AU2, Tahir A1
1
Department of Paediatrics, Usmanu Danfodiyo University Teaching Hospital, PMB 2370, Sokoto, Sokoto State, Nigeria. 2 Department of Obstetrics and Gynaecology, Usmanu Danfodiyo University Teaching Hospital, PMB 2370, Sokoto, Sokoto State, Nigeria. *Corresponding author email: benonankpa@yahoo.com ABSTRACT Diprosopus is an extremely rare form of congenital anomaly that results in partial or total duplication of the face. Most cases of diprosopus are delivered as stillborn or die few moments after delivery. The aim of this report is to alert clinicians that the antenatal finding of polyhydramnious may be strongly associated with fetal diprosopus, this routine high resolution anomaly scans should be recommended to help detect such anomaly early in pregnancy. We report a case of a female neonate with partial duplication of the face (diprosopus) delivered by a 39 year old booked multipara. Babys condition deteriorated within 24hrs with worsening re spiratory distress and died on the 2nd day of life. Key words: Facial diprosopus INTRODUCTION Diprosopus, is a Greek word for two-faced.1 This congenital anomaly is often referred to as craniofacial duplication in which there is partial or total duplication of the face. However, the fetus has a single trunk with normal limbs. In a typical presentation the fetus has a duplicated nose with eyes spaced far apart, but, in extreme cases, the baby has the entire face duplicated (i.e. diprosopus). It is an extremely rare condition with a reported incidence of 1 case in 180,000-15 million births.2 Cases of fetal diprosopus have been reported in Italy3, Germany4, Spain5, Saudi Arabia6, Turkey7 and India.8 To our knowledge this is the second case reported in Nigeria, after the case reported by Ibrahim et al9 Several attempts have been made by several researchers to explain the mechanisms that leads to craniofacial duplication. In the presence of two completely formed, but identical faces, the babies are often referred to as a rare variant of conjoined twins. This mechanism resulting in two faces is considered to have occurred as a result of cranial bifurcation during neurulation of the notochord. 10 Two vertebral axes develop alongside the neural plates as a result of the bifurcation including neural crest derivatives. Facts from the literature also revealed that 0.4 percent of diprosopus is seen in conjoined twins.10 Another possibility is that there could be an increased production of sonic hedgehog (SHH), a protein which is essential for craniofacial patterning during fetal development; this has already been demonstrated in chicks by researchers in an experimental studies.11 These studies showed that the chicks were born with anomalies including double beaks with their eyes spaced far apart. In contrast, the researchers also 461 Onankpa etal., Int J Med Res Health Sci. 2014;3(2):461-463
found that too little SHH led to abnormal midline facial features resulting in cyclopia.11 Prenatal diagnosis is possible for diprosopus using in utero technics including ultrasound and computer tomography (CT) scanning. The presence of polyhdromnios is considered as a strong indication of craniofacial duplication. Presently, there is no treatment for diprosopus however, termination of pregnancy is sometimes considered an option, especially if diagnosed is made early in pregnancy. Children with this defect are normally stillborn, but a young girl, Lali Singh, born in 2008 survived for 2 full months before dying of a heart attack. 12 Partial facial duplication, as in our case, is associated with fewer anomalies, and the prognosis is better with symmetry and an excess of tissue, rather than a deficiency, favoring a positive result. 13 Most of the cases reported were females (4 males/11 females). 5 To our knowledge, there have been less than 150 reports of diprosopus in the world medical literature. 9 CASE REPORT Baby AM, a female was delivered to a 39- year old booked multipara. The mother had regular antenatal visits. The mother was admitted on account of polyhydramnious at 36 weeks gestation. She had abruptio placenta while on admission and, she was delivered of the baby by emergency Caesarean section. Baby required minimal resuscitation, had Apgar scores of 7 & 9 at 1st and 5th minutes respectively. The birth weight was 2800grams, length was 47centimeters and the occipito-frontal circumference was 35centimeters. Baby was uniformly pink, in mild respiratory distress with SPO2 of 98%. The major findings were on the head and neck. Baby had one cranium with 2 faces fused at the midline, with a pair of mouth for each face. The left face had an intact nose with the right face having a trunk like organ with a single opening for a nose. There were 2 intact ears. The left face had a well formed left eye; the other incomplete eye appeared to fuse in a transverse groove across the faces. Each head had an anterior fontanelle. Baby had normal female external genitalia. Babys condition deteriorated within 24hrs with worsening respiratory distress and died on the 2nd day of life. The parents declined autopsy. However, we got an ethical
clearance from UDUTH ethical committee and an informed consent from the parents to report the case.
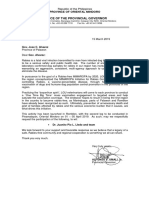
Fig 1: Female neonate with diprosopus DISCUSSION Craniofacial duplication remains a rare entity with only 27 cases reported since 1900.14 Polyhydramnios, a condition that is considered as an indication for craniofacial duplication was detected in this patient. The risk factor for congenital anomaly includes familial tendencies, advance maternal age, previous history and polyhydramnious. The patient was of advance age and developed polyhydramnious during the third trimester. However, repeated ultrasound scan done could not reveal other findings apart from polyhydramnious. Perhaps a high resolution 4D scan would have detected these congenital anomaly and also highlight others if any. Other investigations, including CT-scan, MRI may have helped in the diagnosis, but the cost of this investigation is beyond the reach of most patients in our environment. Congenital anomalies are associated with myths and beliefs, particularly in Africa and sub-Saharan Africa. Thus, such babies are abandoned and poorly cared for by their parents. Probably because diprosopus is rare, few management options including corrective surgeries have been documented.15 The prognosis and fetal outcome has remained unfortunately poor in all cases reported. CONCLUSION Diagnosis may be quite elusive during pregnancy with many cases undetected before delivery. High index of suspicion, full evaluation of cases of polyhydromnious and high resolution scan may help in the early diagnosis and prompt intervention. 462
Onankpa etal.,
Int J Med Res Health Sci. 2014;3(2):461-463
Conflict of interest: None REFERENCES 1. Al Muti Zaitoun A. Chang J, booker M. Doprosopus (Partially duplicated shead) associated with anencephaly. A case report. Pathology Research and Practice. 1999;195:45-50 2. DArmiento, Massimo, Jessica Falleti, Maria Marilotti, Pasquale Mertinelli. Diprosopus Conjoined Twins: Radiologic, Autopic, and Histological Study of a Case. Fetal and Pediatric Pathology. 2010;29:43138 3. Pavone L, Camera G, Grasso S, Gambini C, Barberis M, Garaffo S etal., Diprosopus with associated malformations: report of two cases. Am J Med Genet. 1987;1:85-88 4. Stefan Hhnel, Peter Schramm, Stefan Hassfeld, Hans H Steiner, Angelika Seitz. Craniofacial duplication (diprosopus): CT, MR imaging, and MR angiography findings case report. Radiology. 2003;1:210-3. 5. Mara Luisa Martnez-Fras, Eva Bermejo, Jacobo Mendioroz, Elvira Rodrguez-Pinilla, Manuel Blanco, Javier Egs, Valentn Flix. Epidemiological and clinical analysis of a consecutive series of conjoined twins in Spain. Journal of Pediatric Surgery. 2009; 44(4):811-20 6. Amr SS, Hammouri MF. Craniofacial duplication (diprosopus): report of a case with a review of the literature. Eur J Obstet Gynecol Reprod Biol. 1995;1:77-80 7. Kutsi Koseoglu, Cantay Gok, Yelda Dayanir. CT and MR imaging findings of a rare craniofacial malformation: diprosopus. Am J Roentgenol. 2003;3:863-64 8. Suhil A Choh, Bakshi Jehangir, Naseer A Choh, Omar Kirmani, Roomi Yousuf. Imaging findings in diprosopus tetraophthalmos: a case report. Pediatr Int. 2010;1:54-6 9. Ibrahim A, Mshelbwala PM, Ajike SO, Asuku ME, Ameh EA. Diprosopus (double mouth) in a Nigerian child: Case report and literature review. Nigerian Journal of Plastic Surgery 2012;8(2) 10. Dhaliwal Harjit, Paul Adinkra, Diane Ennis, and Pauline Green. Monocephalus Diprosopus (Complete Craniofacial Duplication) Associated with Hydrancephaly and Other Congenital Anomalies. Priory Lodge Education Limited, 11.
12. 13.
14.
15.
2007. http://priory.com/medicine/Birth_ Abnormality.htm (Accessed November, 16, 2010). Hannel, Stefan, Peter Schramm, Stefan Hassfeld, Hans Steiner, and Angelika Seitz. Craniofacial Duplication (Diprosopus): CT, MR Imaging, and MR Angiography Findings. Radiology.2003;226: 21013 Jamie Frater Top 10 Bizarre Medical Anomalies. LISTVERSE. January 8, 2009. June Wu, David A Staffenberg, John B Mulliken, Alan L Shanske. Diprosopus: a unique case and review of the literature. Teratology. 2002;6:28287 Turpin IM, Furnas DW, Amlie RN. Craniofacial duplication (diprosopus). Plast Reconstr Surg. 1981;67: 139e-42 Okazaki, Joel, James Wilson, Stephen Holmes, Linda Vandermark. Diprosopus: Diagnosis in Utero. American Journal of Roentgenology. 1987;149:14748.
463 Onankpa etal., Int J Med Res Health Sci. 2014;3(2):461-463
You might also like
- Prenatal Diagnosis of Harlequin Ichthyosis: A Case ReportDocument4 pagesPrenatal Diagnosis of Harlequin Ichthyosis: A Case Reportcitra annisa fitriNo ratings yet
- Thanatoporic Dysplasia FIXDocument7 pagesThanatoporic Dysplasia FIXYudha GanesaNo ratings yet
- Ultrasound Diagnosis of Facial Anomalies (Diagnosis Usg Untuk Kelainan Wajah)Document7 pagesUltrasound Diagnosis of Facial Anomalies (Diagnosis Usg Untuk Kelainan Wajah)Puspita SariNo ratings yet
- Goldenhar PDFDocument4 pagesGoldenhar PDFDaniel FernandezNo ratings yet
- Congenital Anophthalmos in Benin CityDocument3 pagesCongenital Anophthalmos in Benin CityLjubomirErdoglijaNo ratings yet
- An Insight Into - Hemifacial MicrosomiaDocument6 pagesAn Insight Into - Hemifacial MicrosomiaIJAR JOURNALNo ratings yet
- Cervical AuricleDocument2 pagesCervical AuricleTahir S.MNo ratings yet
- AnencephalyDocument6 pagesAnencephalyMetta SariNo ratings yet
- Craniopharyngioma Revealed by Papilledema in A Child: A Case ReportDocument4 pagesCraniopharyngioma Revealed by Papilledema in A Child: A Case ReportIJAR JOURNALNo ratings yet
- Voss 2018Document6 pagesVoss 2018lupalladiniNo ratings yet
- CebocephalyDocument12 pagesCebocephalyUser AbNo ratings yet
- AMS PublishedDocument4 pagesAMS PublishedAyanawNo ratings yet
- 40 Odogu EtalDocument4 pages40 Odogu EtaleditorijmrhsNo ratings yet
- Accepted Manuscript: Epilepsy ResearchDocument25 pagesAccepted Manuscript: Epilepsy ResearchasfwegereNo ratings yet
- Case Reports Esophageal Foreign Body in NeonatesDocument3 pagesCase Reports Esophageal Foreign Body in NeonatesmuhammadpanggihpangestuNo ratings yet
- Congenital Rubella Syndrome Global IssueDocument1 pageCongenital Rubella Syndrome Global IssueAnonymous mhsYKgCNo ratings yet
- Should We Say NO To Body Piercing in Children? Complications After Ear Piercing in ChildrenDocument3 pagesShould We Say NO To Body Piercing in Children? Complications After Ear Piercing in ChildrenGhalyRizqiMauludinNo ratings yet
- Santos Et Al 2011. Hearing Loss and Airway Problems in Children With MucopolysaccharidosesDocument7 pagesSantos Et Al 2011. Hearing Loss and Airway Problems in Children With MucopolysaccharidosesBoNo ratings yet
- Goldenhar Syndrome An Ophthalmological Perspective: A Case SeriesDocument6 pagesGoldenhar Syndrome An Ophthalmological Perspective: A Case SeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- HerlequinDocument4 pagesHerlequinOman ArifNo ratings yet
- Congenital Toxoplasmosis Associated With Severe Intracerebral Calcification and West SyndromeDocument3 pagesCongenital Toxoplasmosis Associated With Severe Intracerebral Calcification and West SyndromeDevina Rossita HapsariNo ratings yet
- Achondroplasia: September 2012Document7 pagesAchondroplasia: September 2012ancillaagrayn100% (1)
- Bilateral Blindness Due To Pterygium - A Case ReportDocument3 pagesBilateral Blindness Due To Pterygium - A Case ReportDavid Al HavizNo ratings yet
- International Journal of Research in Pharmaceutical SciencesDocument12 pagesInternational Journal of Research in Pharmaceutical SciencesMagfirah AliyyaNo ratings yet
- Anophthalmia WikiDocument7 pagesAnophthalmia WikiUnggul YudhaNo ratings yet
- Congenital Rubella Syndrome: It Still Exists in India: Abst TDocument2 pagesCongenital Rubella Syndrome: It Still Exists in India: Abst TTara KentNo ratings yet
- Ankyloblepharon Filiforme Adnatum: A Case ReportDocument4 pagesAnkyloblepharon Filiforme Adnatum: A Case ReportGheavita Chandra DewiNo ratings yet
- MIIASEDocument5 pagesMIIASEcha_09No ratings yet
- Diagnóstico Tardio de MARDocument8 pagesDiagnóstico Tardio de MARthedoctor1986No ratings yet
- Final Case Report FinalDocument7 pagesFinal Case Report FinalPawan JarwalNo ratings yet
- When Fryn Met Edward Two Rare Syndromes in A 2022 Medical Journal Armed ForDocument4 pagesWhen Fryn Met Edward Two Rare Syndromes in A 2022 Medical Journal Armed ForAnisha RanaNo ratings yet
- Pediatrics 2005 Trotter 771 83Document16 pagesPediatrics 2005 Trotter 771 83Ligia RiosNo ratings yet
- Ptriase em CiliosDocument4 pagesPtriase em CiliosRafael CedroNo ratings yet
- Contribution of Ultrasound in The Diagnosis of Thanatophore Dysplasia:about A Case in BamakoDocument4 pagesContribution of Ultrasound in The Diagnosis of Thanatophore Dysplasia:about A Case in BamakoIJAR JOURNALNo ratings yet
- Intra-Aural Tick Induced Facial PalsyDocument2 pagesIntra-Aural Tick Induced Facial PalsyAssaye NibretNo ratings yet
- Sirenomelia: A Case Report of A Rare Congenital Anamaly and Review of LiteratureDocument3 pagesSirenomelia: A Case Report of A Rare Congenital Anamaly and Review of LiteratureInt Journal of Recent Surgical and Medical SciNo ratings yet
- Spinal DisDocument32 pagesSpinal DisAkmal Niam FirdausiNo ratings yet
- Interdisciplinary Neurosurgery: Jimmy Ntimbani, Adrian Kelly, Patrick Lekgwara TDocument4 pagesInterdisciplinary Neurosurgery: Jimmy Ntimbani, Adrian Kelly, Patrick Lekgwara TKunni MardhiyahNo ratings yet
- 292-Article Text-1640-1-10-20190515Document8 pages292-Article Text-1640-1-10-20190515Liset Edreira Cutipa SallucaNo ratings yet
- European Journal of Medical GeneticsDocument6 pagesEuropean Journal of Medical GeneticsLarissa DmtNo ratings yet
- Journal of Diagnostic Medical Sonography 2010 Moore 286 9Document4 pagesJournal of Diagnostic Medical Sonography 2010 Moore 286 9Hanarisha Putri AzkiaNo ratings yet
- Congenital Hydrocephalus Prevalence Prenatal DiagnosisDocument6 pagesCongenital Hydrocephalus Prevalence Prenatal DiagnosisnendaayuwandariNo ratings yet
- Clinical Manifestations of Ocular Toxoplasmosis in Yogyakarta, Indonesia: A Clinical Review of 173 CasesDocument7 pagesClinical Manifestations of Ocular Toxoplasmosis in Yogyakarta, Indonesia: A Clinical Review of 173 CasesRiza Haida WardhaniNo ratings yet
- Epulis KongenitalDocument3 pagesEpulis KongenitalFriadi NataNo ratings yet
- Spina Bifida Guide: Types, Causes & Nursing CareDocument5 pagesSpina Bifida Guide: Types, Causes & Nursing CareJulliza Joy PandiNo ratings yet
- Role of Diagnostic Laparoscopy in The Management of Gastro Oesophageal, Pancreatic and Colorectal CancersDocument3 pagesRole of Diagnostic Laparoscopy in The Management of Gastro Oesophageal, Pancreatic and Colorectal CancersIOSRjournalNo ratings yet
- BurgDocument16 pagesBurgGrazyele SantanaNo ratings yet
- Congenital Rubella Syndrome-Case ReportDocument4 pagesCongenital Rubella Syndrome-Case ReportErlina WahyuNo ratings yet
- The "Epidemic" of Occipital Flattening: Why It Is Happening and What To Do About ItDocument5 pagesThe "Epidemic" of Occipital Flattening: Why It Is Happening and What To Do About ItDinner and a Donkey Show TheatreNo ratings yet
- Nihms964774 DiagnostikDocument33 pagesNihms964774 Diagnostikandi ilmansyahNo ratings yet
- Case ReportDocument6 pagesCase ReportJellie MendozaNo ratings yet
- Neural Tube Defects: Group 1Document28 pagesNeural Tube Defects: Group 1imneverwrong2492100% (1)
- Frontal Encephalocele - A Rare Case Report With Review of LiteratureDocument4 pagesFrontal Encephalocele - A Rare Case Report With Review of LiteratureAyu TrisyaNo ratings yet
- Case Report on Peters' Plus Syndrome with Bilateral SclerocorneaDocument14 pagesCase Report on Peters' Plus Syndrome with Bilateral SclerocorneaAaron Lemuel OngNo ratings yet
- FTPDocument2 pagesFTPDesta FransiscaNo ratings yet
- Case Report For Case Presentations Short Rib Polydactyly SyndromeDocument8 pagesCase Report For Case Presentations Short Rib Polydactyly Syndromeapi-390240132No ratings yet
- s-0043-1764179Document5 pagess-0043-1764179Phong HoàngNo ratings yet
- Etiology of Proptosis in Children Sindhu 1998Document3 pagesEtiology of Proptosis in Children Sindhu 1998Putri Wulan SukmawatiNo ratings yet
- Ijmrhs Vol 4 Issue 4Document193 pagesIjmrhs Vol 4 Issue 4editorijmrhs0% (1)
- Ijmrhs Vol 1 Issue 1Document257 pagesIjmrhs Vol 1 Issue 1editorijmrhsNo ratings yet
- Ijmrhs Vol 3 Issue 1Document228 pagesIjmrhs Vol 3 Issue 1editorijmrhsNo ratings yet
- Ijmrhs Vol 4 Issue 2Document219 pagesIjmrhs Vol 4 Issue 2editorijmrhsNo ratings yet
- Ijmrhs Vol 4 Issue 3Document263 pagesIjmrhs Vol 4 Issue 3editorijmrhsNo ratings yet
- Ijmrhs Vol 3 Issue 3Document271 pagesIjmrhs Vol 3 Issue 3editorijmrhsNo ratings yet
- Ijmrhs Vol 3 Issue 4Document294 pagesIjmrhs Vol 3 Issue 4editorijmrhsNo ratings yet
- Ijmrhs Vol 2 Issue 3Document399 pagesIjmrhs Vol 2 Issue 3editorijmrhs100% (1)
- 48 MakrandDocument2 pages48 MakrandeditorijmrhsNo ratings yet
- Ijmrhs Vol 2 Issue 1Document110 pagesIjmrhs Vol 2 Issue 1editorijmrhs100% (1)
- 47serban Turliuc EtalDocument4 pages47serban Turliuc EtaleditorijmrhsNo ratings yet
- Ijmrhs Vol 1 Issue 1Document257 pagesIjmrhs Vol 1 Issue 1editorijmrhsNo ratings yet
- Ijmrhs Vol 3 Issue 2Document281 pagesIjmrhs Vol 3 Issue 2editorijmrhsNo ratings yet
- Ijmrhs Vol 2 Issue 4Document321 pagesIjmrhs Vol 2 Issue 4editorijmrhsNo ratings yet
- 43chaitali EtalDocument3 pages43chaitali EtaleditorijmrhsNo ratings yet
- Ijmrhs Vol 2 Issue 2Document197 pagesIjmrhs Vol 2 Issue 2editorijmrhsNo ratings yet
- Recurrent Cornual Ectopic Pregnancy - A Case Report: Article InfoDocument2 pagesRecurrent Cornual Ectopic Pregnancy - A Case Report: Article InfoeditorijmrhsNo ratings yet
- 41anurag EtalDocument2 pages41anurag EtaleditorijmrhsNo ratings yet
- 45mohit EtalDocument4 pages45mohit EtaleditorijmrhsNo ratings yet
- Williams-Campbell Syndrome-A Rare Entity of Congenital Bronchiectasis: A Case Report in AdultDocument3 pagesWilliams-Campbell Syndrome-A Rare Entity of Congenital Bronchiectasis: A Case Report in AdulteditorijmrhsNo ratings yet
- Pernicious Anemia in Young: A Case Report With Review of LiteratureDocument5 pagesPernicious Anemia in Young: A Case Report With Review of LiteratureeditorijmrhsNo ratings yet
- 38vaishnavi EtalDocument3 pages38vaishnavi EtaleditorijmrhsNo ratings yet
- 36rashmipal EtalDocument6 pages36rashmipal EtaleditorijmrhsNo ratings yet
- 35krishnasamy EtalDocument1 page35krishnasamy EtaleditorijmrhsNo ratings yet
- 37poflee EtalDocument3 pages37poflee EtaleditorijmrhsNo ratings yet
- 40vedant EtalDocument4 pages40vedant EtaleditorijmrhsNo ratings yet
- 34tupe EtalDocument5 pages34tupe EtaleditorijmrhsNo ratings yet
- 32bheemprasad EtalDocument3 pages32bheemprasad EtaleditorijmrhsNo ratings yet
- 33 Prabu RamDocument5 pages33 Prabu RameditorijmrhsNo ratings yet
- Placental AbnormalitiesDocument3 pagesPlacental AbnormalitiesThakoon TtsNo ratings yet
- Emteaz OphthalmologyDocument16 pagesEmteaz OphthalmologyRaouf Ra'fat SolimanNo ratings yet
- Suspected Adverse Reactions To COVID 19 Vaccination and Safety of SoHODocument11 pagesSuspected Adverse Reactions To COVID 19 Vaccination and Safety of SoHOVevveNo ratings yet
- Tablet binders and excipientsDocument30 pagesTablet binders and excipientsmary navalNo ratings yet
- Role of Autologous Platelet-Rich Plasma in Z-PlastyDocument3 pagesRole of Autologous Platelet-Rich Plasma in Z-PlastyasclepiuspdfsNo ratings yet
- Wolford2017 STO - Surgical Planning in Orthognathic SurgeryDocument79 pagesWolford2017 STO - Surgical Planning in Orthognathic SurgeryandresNo ratings yet
- 1 Dental Caries PDFDocument38 pages1 Dental Caries PDFmayang putriNo ratings yet
- Home: Correspondence:: PubmedDocument23 pagesHome: Correspondence:: PubmedArjun ShawNo ratings yet
- Perceptions About Childhood Vaccinations: Pam CooperDocument19 pagesPerceptions About Childhood Vaccinations: Pam CooperLancasterOnlineNo ratings yet
- Banned Drugs in IndiaDocument3 pagesBanned Drugs in IndiaGottumukkala Venkateswara RaoNo ratings yet
- 1 s2.0 S0828282X22001271 MainDocument11 pages1 s2.0 S0828282X22001271 MainLilianne Mbengani LaranjeiraNo ratings yet
- Ashley Fagert ResumeDocument1 pageAshley Fagert Resumeapi-455767165No ratings yet
- Aids 2013Document404 pagesAids 2013kovaron80No ratings yet
- (Helveston) Surgical Management of StrabismusDocument518 pages(Helveston) Surgical Management of StrabismusMarianaNo ratings yet
- ABO Blood Type Incompatibilty (Super Final)Document58 pagesABO Blood Type Incompatibilty (Super Final)Marc Michael Dela CruzNo ratings yet
- HydramniosDocument31 pagesHydramniosSpandana DepuruNo ratings yet
- CH - 05 - SW CorrectedDocument10 pagesCH - 05 - SW CorrectedHenok BayuNo ratings yet
- Detoxification and Chelation Protocols GuideDocument213 pagesDetoxification and Chelation Protocols Guidedoggydog100% (3)
- ICU Insulin Infusion ProtocolDocument4 pagesICU Insulin Infusion ProtocolWeeranan Sueb-LaNo ratings yet
- File - 20190927 - 153306 - Drugs Reaction 2019Document410 pagesFile - 20190927 - 153306 - Drugs Reaction 2019ntnquynhpro100% (1)
- Varicose VeinsDocument12 pagesVaricose Veinscheo sealyNo ratings yet
- (Book 4) Collins Parker, Mia - PCOS Nutrition - A Complete PCOS Diet Book With 4 Week Meal Plan and 4 Week Fitness Exercise Plan To Reduce Weight and Prevent Diabetes. PCOS Causes, Symptoms and HolDocument134 pages(Book 4) Collins Parker, Mia - PCOS Nutrition - A Complete PCOS Diet Book With 4 Week Meal Plan and 4 Week Fitness Exercise Plan To Reduce Weight and Prevent Diabetes. PCOS Causes, Symptoms and HolAndreea Daniela100% (4)
- Hiatal HerniaDocument9 pagesHiatal HerniaAnnJenn AsideraNo ratings yet
- Office of The Provincial Governor: Province of Oriental MindoroDocument1 pageOffice of The Provincial Governor: Province of Oriental MindoroZyreen Kate BCNo ratings yet
- OCD Children AdolescentsDocument8 pagesOCD Children AdolescentsCésar CorveraNo ratings yet
- Case Notes: Requesting Home Care for Robyn HarwoodDocument3 pagesCase Notes: Requesting Home Care for Robyn Harwoodiduhilag75% (8)
- First Aid Guide for WorkplacesDocument40 pagesFirst Aid Guide for WorkplaceswwwNo ratings yet
- Mri Signa Ge Book PDFDocument74 pagesMri Signa Ge Book PDFDicky YkcidNo ratings yet
- Aden Abdi-ResumeDocument2 pagesAden Abdi-Resumeapi-534490436No ratings yet
- 310-Article Text-582-1-10-20210312-1Document13 pages310-Article Text-582-1-10-20210312-1Ni Putu SwastyNo ratings yet