You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Odors of Santity Distinctions of The Holy in Early Christianity and IslamDocument13 pagesOdors of Santity Distinctions of The Holy in Early Christianity and Islamkiedd_04100% (1)
- Cell PhysiologyDocument61 pagesCell Physiologykiedd_04100% (4)
- Microsoft Word Document جديدDocument3 pagesMicrosoft Word Document جديدHisham EssamNo ratings yet
- The Place For Others in IslamDocument27 pagesThe Place For Others in Islamkiedd_04No ratings yet
- "Traditional" Exegeses of Q 4:34Document15 pages"Traditional" Exegeses of Q 4:34kiedd_04No ratings yet
- Iklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012Document2 pagesIklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012kiedd_04No ratings yet
- Refleks ArcsDocument34 pagesRefleks Arcskiedd_04100% (1)
- SYNAPSEDocument35 pagesSYNAPSEkiedd_04100% (3)
- From The Bodies of Bees Classical and Christian Echoes in Surah Al-NahlDocument25 pagesFrom The Bodies of Bees Classical and Christian Echoes in Surah Al-Nahlkiedd_04No ratings yet
- Microbiology Colour Plate No.6Document1 pageMicrobiology Colour Plate No.6kiedd_04No ratings yet
- Microbiology Colour Plate No.7Document1 pageMicrobiology Colour Plate No.7kiedd_04No ratings yet
- Microbiology Colour Plate No.5Document1 pageMicrobiology Colour Plate No.5kiedd_04No ratings yet
- Microbiology Colour Plate No.8Document1 pageMicrobiology Colour Plate No.8kiedd_04No ratings yet
- Fadhilat Surah at TakwirDocument1 pageFadhilat Surah at Takwirkiedd_04No ratings yet
- Microbiology Colour Plate No.9Document1 pageMicrobiology Colour Plate No.9kiedd_04No ratings yet
- API® CoryneDocument4 pagesAPI® Corynekiedd_04No ratings yet
- Microbiology Colour Plate No.2Document1 pageMicrobiology Colour Plate No.2kiedd_04No ratings yet
- Microbiology Colour Plate No.1Document1 pageMicrobiology Colour Plate No.1kiedd_04No ratings yet
- Microbiology Colour Plate No.4Document1 pageMicrobiology Colour Plate No.4kiedd_04No ratings yet
- Mitigation of Climate ChangeDocument41 pagesMitigation of Climate Changekiedd_04No ratings yet
- Microbiology Colour Plate No.3Document1 pageMicrobiology Colour Plate No.3kiedd_04No ratings yet
- Advance Diagnostic Medical Laboratory: The AP 20E® For Identification of BacteriaDocument1 pageAdvance Diagnostic Medical Laboratory: The AP 20E® For Identification of Bacteriakiedd_04100% (1)
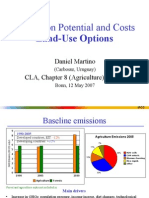
- Mitigation Potential and Costs Land-Use OptionsDocument9 pagesMitigation Potential and Costs Land-Use Optionskiedd_04No ratings yet
- Diagram of Classification of EnterobacteriaDocument1 pageDiagram of Classification of Enterobacteriakiedd_04100% (1)
- Mitigation of Climate ChangeDocument25 pagesMitigation of Climate Changekiedd_04No ratings yet
- Carnitine DeficiencyDocument21 pagesCarnitine Deficiencykiedd_04100% (1)
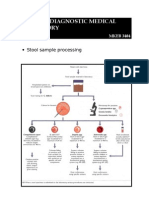
- Stool Sample ProcessingDocument1 pageStool Sample Processingkiedd_04No ratings yet
- Philosophical Consolation in Christianity and Islam Boethious and Al-KindiDocument10 pagesPhilosophical Consolation in Christianity and Islam Boethious and Al-Kindikiedd_04No ratings yet
- Oxidase TestDocument1 pageOxidase Testkiedd_04100% (1)
- Insulin Therapy in Type 1 Diabetes UpdateDocument83 pagesInsulin Therapy in Type 1 Diabetes UpdateasupicuNo ratings yet
- Surgical Managment of DMDocument42 pagesSurgical Managment of DMHaroon Malik100% (1)
- Diabetic KetoacidosisDocument21 pagesDiabetic KetoacidosisDrishti ShresthaNo ratings yet
- Etiology of Type 2 Diabetes PDFDocument2 pagesEtiology of Type 2 Diabetes PDFJustinNo ratings yet
- DiabetesDocument32 pagesDiabetesaneeshajaiswalNo ratings yet
- Endometab Exam 2018Document8 pagesEndometab Exam 2018teabagmanNo ratings yet
- Public Health FinalDocument13 pagesPublic Health FinalAbeyOdunugaQudusNo ratings yet
- WC 500029819Document23 pagesWC 500029819nsk79in@gmail.comNo ratings yet
- Edexcel International Gcse Biology Question Practice Biology Paper 2 Sample PagesDocument72 pagesEdexcel International Gcse Biology Question Practice Biology Paper 2 Sample PagesAaron SandhuNo ratings yet
- Diabetes R&DDocument132 pagesDiabetes R&Dlali62No ratings yet
- NCLEX RN Practice Questions 17Document29 pagesNCLEX RN Practice Questions 17clarheena89% (9)
- Diabetes MallitusDocument33 pagesDiabetes Mallitushammu hothi100% (2)
- Diabetes MellitusDocument8 pagesDiabetes MellitusJaja RamosNo ratings yet
- Insulin Case Studies AACE 5-20-05Document56 pagesInsulin Case Studies AACE 5-20-05Leanne Shepherd100% (2)
- Diabetes Mellitus PathologyDocument5 pagesDiabetes Mellitus PathologyNada MuchNo ratings yet
- Diabetic NephropathyDocument317 pagesDiabetic Nephropathy'sally' RosaLie EllyNo ratings yet
- Diabetes BrochureDocument3 pagesDiabetes Brochureapi-348372254No ratings yet
- Humalog - Uses, Dosage & Side Effects - DrugsDocument4 pagesHumalog - Uses, Dosage & Side Effects - Drugsremyde07100% (1)
- Process PaperDocument18 pagesProcess Paperapi-283957261No ratings yet
- Emphasis of Yoga in The Management of Diabetes 2155 6156 1000613Document11 pagesEmphasis of Yoga in The Management of Diabetes 2155 6156 1000613AnuradhatagoreNo ratings yet
- A P Research Paper DiabetesDocument8 pagesA P Research Paper Diabetesapi-353042837No ratings yet
- Diabetes MellitusDocument42 pagesDiabetes MellitusLyza Fernandez AlbotraNo ratings yet
- Edmund Silvania (Antidiabetic)Document12 pagesEdmund Silvania (Antidiabetic)James WilliamNo ratings yet
- A Client With Type 1 Diabetes: Nursing Care PlanDocument1 pageA Client With Type 1 Diabetes: Nursing Care Plankimchi girlNo ratings yet
- Diagnosis and Treatment of Diabetes Mellitus in Chronic PancreatitisDocument7 pagesDiagnosis and Treatment of Diabetes Mellitus in Chronic PancreatitisFarid TaufiqNo ratings yet
- 03 Chapter 2Document0 pages03 Chapter 2Charles Amaechi100% (1)
- Herbal AntidiabeticsDocument8 pagesHerbal Antidiabeticstio_bsNo ratings yet
- Diabetic Foot Case PresentationDocument58 pagesDiabetic Foot Case PresentationMissoSandoqji100% (1)
- Insulin and Oral Hypoglycemic AgentsDocument27 pagesInsulin and Oral Hypoglycemic Agentsapi-19916399100% (1)