You might also like
- Application For Assistance Under The Supreme Court Health and Welfare Plan (Revised - 2010)Document3 pagesApplication For Assistance Under The Supreme Court Health and Welfare Plan (Revised - 2010)Eunice Navarro100% (2)
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsFrom EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex 2 List of Procedure Case RatesDocument98 pagesPhilHealth Circular No. 0035, s.2013 Annex 2 List of Procedure Case RatesChrysanthus Herrera50% (2)
- 3 - Speaking All Needed Notes PDFDocument165 pages3 - Speaking All Needed Notes PDFMic Atef86% (7)
- Philhealth cf4Document6 pagesPhilhealth cf4Jose AcuinNo ratings yet
- Claim Form Dd2642Document4 pagesClaim Form Dd2642Adina BusteaNo ratings yet
- Maxicare Reimbursement Claim Form PDFDocument1 pageMaxicare Reimbursement Claim Form PDFJolina de VeraNo ratings yet
- CF1Document1 pageCF1Kim ViñasNo ratings yet
- Afghan - Summary of PPP Hospitals Feasibility Studies - FINALDocument36 pagesAfghan - Summary of PPP Hospitals Feasibility Studies - FINALborn2prayNo ratings yet
- NYP Website Info - CoursesDocument15 pagesNYP Website Info - CoursesYuda FhunkshyangNo ratings yet
- PhilHealth - ClaimForm2 1Document2 pagesPhilHealth - ClaimForm2 1Harold Kirby TanNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex11 - GuidelinesOnTheProperAccomplishmentOfClaimForm2 (November2013)Document8 pagesPhilHealth Circular No. 0035, s.2013 Annex11 - GuidelinesOnTheProperAccomplishmentOfClaimForm2 (November2013)Chrysanthus HerreraNo ratings yet
- Claims Reimbursement Form (For MRC) : Member General InformationDocument2 pagesClaims Reimbursement Form (For MRC) : Member General Informationathenixia100% (2)
- PhilHealth ClaimForm2Document2 pagesPhilHealth ClaimForm2La Lolls CruzNo ratings yet
- Claim Form NewDocument4 pagesClaim Form Newparvazahmed03191No ratings yet
- Claims Reimbursement Form: Member General InformationDocument1 pageClaims Reimbursement Form: Member General InformationFirmament DevelopmentNo ratings yet
- Claims Reimbursement Form: Member General InformationDocument1 pageClaims Reimbursement Form: Member General InformationHarold TanNo ratings yet
- SITEL - Claims Reimbursement Form Rev.06 PDFDocument2 pagesSITEL - Claims Reimbursement Form Rev.06 PDFJoyce HerreraNo ratings yet
- Claim FormDocument4 pagesClaim Formdharani633No ratings yet
- COVID-19 Test Claim Form - 23122020 Woking File - ENG - FinalDocument2 pagesCOVID-19 Test Claim Form - 23122020 Woking File - ENG - FinalnorhanaaNo ratings yet
- Claim Form IHealthcareDocument5 pagesClaim Form IHealthcarePradeep Kumar VupalaNo ratings yet
- Claims Reimbursement Form PDFDocument2 pagesClaims Reimbursement Form PDFokong bokongNo ratings yet
- Bajaj Allianz Cashless Request FormDocument3 pagesBajaj Allianz Cashless Request FormM/s MicrotechNo ratings yet
- Family Planning Manual Indemnity SchemeDocument10 pagesFamily Planning Manual Indemnity SchemeRamdas SalveNo ratings yet
- Claim FormDocument3 pagesClaim FormKhameer L Shah100% (1)
- Mumbai Claim FormDocument5 pagesMumbai Claim FormsunsangraNo ratings yet
- QCIDocument27 pagesQCIerpNo ratings yet
- Philhealth BenefitsDocument2 pagesPhilhealth BenefitsjohnhenryvNo ratings yet
- Rev 3 RAWAT JALAN INDIVIDUAL InggrisDocument2 pagesRev 3 RAWAT JALAN INDIVIDUAL InggrisمولديياNo ratings yet
- Cashless Request FormDocument4 pagesCashless Request FormManish RanjanNo ratings yet
- BCBSTX Halliburton Intl Claim FormDocument2 pagesBCBSTX Halliburton Intl Claim FormLoganBohannonNo ratings yet
- Medical Reibursement Proposal Form SetDocument5 pagesMedical Reibursement Proposal Form SetSharath VaddiparthiNo ratings yet
- Covid-19 Test Claim FormDocument2 pagesCovid-19 Test Claim Formmuhammad anasNo ratings yet
- SG Worldcare Pre AuthorisationDocument3 pagesSG Worldcare Pre Authorisationbernardlim86No ratings yet
- Medical Inpatient ProformaDocument6 pagesMedical Inpatient ProformapenusilaNo ratings yet
- Health Insurance Claim FormDocument3 pagesHealth Insurance Claim FormdivechahimanshuNo ratings yet
- CLAIMS REIMBURSEMENT FORM EditedDocument1 pageCLAIMS REIMBURSEMENT FORM EditedOliver SyNo ratings yet
- Ahmedabad Claim FormDocument5 pagesAhmedabad Claim FormFirdaus PanthakyNo ratings yet
- EPAF - Top Up Request FormDocument2 pagesEPAF - Top Up Request FormMil MalarNo ratings yet
- OPD Form IHealthcare-2Document2 pagesOPD Form IHealthcare-2Masoom Kazmi100% (1)
- BIN Claim Form 1611v11 D PDFDocument5 pagesBIN Claim Form 1611v11 D PDFAnonymous BZF0QIjDNo ratings yet
- Frequently Asked Questions: Claims and BenefitsDocument4 pagesFrequently Asked Questions: Claims and BenefitsjaimeelynpNo ratings yet
- The Oriental Insurance Company Limited (Incorporated in India, Subsidiary of General Insurance Corporation of India)Document4 pagesThe Oriental Insurance Company Limited (Incorporated in India, Subsidiary of General Insurance Corporation of India)Mcnet WideNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument4 pagesClaim Form - Part A' To 'Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part Auser4timepass6237No ratings yet
- Health PDFDocument25 pagesHealth PDFShurieUNo ratings yet
- AXA Reimbursement Form ALL enDocument2 pagesAXA Reimbursement Form ALL enReynard Delos SantosNo ratings yet
- CLAIM FORM Maternity MEAF RSA 69041 3Document5 pagesCLAIM FORM Maternity MEAF RSA 69041 3Arindam ChangdarNo ratings yet
- Claims Reimbursement Form (For MRC) : Member General Information (Required)Document2 pagesClaims Reimbursement Form (For MRC) : Member General Information (Required)lecky youNo ratings yet
- Out-Patient Claim Form: To Be Filled by The PatientDocument2 pagesOut-Patient Claim Form: To Be Filled by The PatientJohanessNo ratings yet
- Existing ADNIC Reimbursement ClaimFormDocument3 pagesExisting ADNIC Reimbursement ClaimFormmohammad loai sabbaghNo ratings yet
- Reimbursement of Medical Claims PDFDocument10 pagesReimbursement of Medical Claims PDFashutosh tiwariNo ratings yet
- Abbott Diabetes Care (PDF Library)Document2 pagesAbbott Diabetes Care (PDF Library)RINA.No ratings yet
- Phil Health ClaimForm GuidelinesDocument7 pagesPhil Health ClaimForm GuidelinesFerdinand CordovizNo ratings yet
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- Newman's Billing and Coding Technicians Study GuideFrom EverandNewman's Billing and Coding Technicians Study GuideRating: 4.5 out of 5 stars4.5/5 (2)
- Health Care Reform Act: Critical Tax and Insurance RamificationsFrom EverandHealth Care Reform Act: Critical Tax and Insurance RamificationsNo ratings yet
- A Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsFrom EverandA Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsNo ratings yet
- How to Enroll in Medicare Health Insurance: Choose a Medicare Part D Drug Plan and a Medicare Supplement PlanFrom EverandHow to Enroll in Medicare Health Insurance: Choose a Medicare Part D Drug Plan and a Medicare Supplement PlanNo ratings yet
- Textbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipFrom EverandTextbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipNo ratings yet
- Medical Plan Forensics: Examining the EvidenceFrom EverandMedical Plan Forensics: Examining the EvidenceNo ratings yet
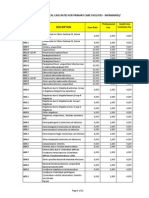
- PhilHealth Circular No. 0035, s.2013 Annex 6 List of Procedure CaseRates For Primary Care FacilitiesDocument22 pagesPhilHealth Circular No. 0035, s.2013 Annex 6 List of Procedure CaseRates For Primary Care FacilitiesChrysanthus Herrera100% (2)
- PhilHealth Circular No. 0035, s.2013 Annex 10 List of Alternative Documents For Record of Operative or Surgical TechniqueDocument14 pagesPhilHealth Circular No. 0035, s.2013 Annex 10 List of Alternative Documents For Record of Operative or Surgical TechniqueChrysanthus HerreraNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex 1 List of Medical Case RatesDocument111 pagesPhilHealth Circular No. 0035, s.2013 Annex 1 List of Medical Case RatesChrysanthus Herrera80% (5)
- PhilHealth Circular No. 0035, s.2013 Annex 4 Examples and Scenarios For The All Case Rates Implementing GuidelinesDocument7 pagesPhilHealth Circular No. 0035, s.2013 Annex 4 Examples and Scenarios For The All Case Rates Implementing GuidelinesChrysanthus HerreraNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesDocument22 pagesPhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesChrysanthus HerreraNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex 3 List of Medical Conditions and Procedures Allowed As Second Case RateDocument31 pagesPhilHealth Circular No. 0035, s.2013 Annex 3 List of Medical Conditions and Procedures Allowed As Second Case RateChrysanthus Herrera0% (1)
- PhilHealth Circular No. 0035, s.2013 Annex 8 List of Medical Conditions Allowed For Referral PackageDocument7 pagesPhilHealth Circular No. 0035, s.2013 Annex 8 List of Medical Conditions Allowed For Referral PackageChrysanthus HerreraNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex 9 Referral FormDocument1 pagePhilHealth Circular No. 0035, s.2013 Annex 9 Referral FormChrysanthus Herrera100% (1)
- PhilHealth Circular No. 0035, s.2013 Annex 7 List of Procedures With LateralityDocument11 pagesPhilHealth Circular No. 0035, s.2013 Annex 7 List of Procedures With LateralityChrysanthus HerreraNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex11 - GuidelinesOnTheProperAccomplishmentOfClaimForm2 (November2013)Document8 pagesPhilHealth Circular No. 0035, s.2013 Annex11 - GuidelinesOnTheProperAccomplishmentOfClaimForm2 (November2013)Chrysanthus HerreraNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex11 PhilHealthClaimForm3 Frontpage (RevisedNovember2013)Document2 pagesPhilHealth Circular No. 0035, s.2013 Annex11 PhilHealthClaimForm3 Frontpage (RevisedNovember2013)Chrysanthus HerreraNo ratings yet
- Philippine Health Insurance Corporation Circular No. 0035, S. 2013 - Implementing Guidelines On The Medical and Procedure Case RatesDocument17 pagesPhilippine Health Insurance Corporation Circular No. 0035, S. 2013 - Implementing Guidelines On The Medical and Procedure Case RatesChrysanthus HerreraNo ratings yet
- Trauma and Stressor-Related DisorderDocument18 pagesTrauma and Stressor-Related DisorderlaehaaaNo ratings yet
- Thyroid Disorders SeminarDocument86 pagesThyroid Disorders SeminarsmrutuNo ratings yet
- Question Papers Forensic Medicine (PG)Document12 pagesQuestion Papers Forensic Medicine (PG)Kumar KP67% (3)
- Traction NursingDocument75 pagesTraction NursingSujith KuttanNo ratings yet
- PQCNC: Hypertension in PregnancyDocument79 pagesPQCNC: Hypertension in PregnancykcochranNo ratings yet
- Uveitis - Treatment - UpToDateDocument12 pagesUveitis - Treatment - UpToDateRohit RajeevanNo ratings yet
- Learning Plan - Semester 3Document2 pagesLearning Plan - Semester 3api-314700318No ratings yet
- ATLSDocument22 pagesATLSHemant Khambhati78% (9)
- Horticultural Therapy Fact Sheet - Rutgers Cook CollegeDocument2 pagesHorticultural Therapy Fact Sheet - Rutgers Cook CollegeKritikou1547100% (1)
- PiperacillinDocument3 pagesPiperacillinMario Magtaka0% (1)
- Arachnoid Granulations PDFDocument5 pagesArachnoid Granulations PDFsebacosNo ratings yet
- Field Triage in TraumaDocument12 pagesField Triage in TraumaKABERA RENENo ratings yet
- Quality and Safety Education For Advanced Nursing Practice - 2009 - Nursing Outlook PDFDocument11 pagesQuality and Safety Education For Advanced Nursing Practice - 2009 - Nursing Outlook PDFrnrmmanphdNo ratings yet
- Oncology-Study of Cancer Cellular AbberationDocument43 pagesOncology-Study of Cancer Cellular AbberationIrwan M. IskoberNo ratings yet
- Administering Blood TransfusionDocument10 pagesAdministering Blood Transfusionkatz_hotchickNo ratings yet
- MRCP Book 070709Document11 pagesMRCP Book 070709wwwrgrobinNo ratings yet
- Call Center Feasibility Study Template4Document17 pagesCall Center Feasibility Study Template4Elvis DsouzaNo ratings yet
- Drug Round - DigoxinDocument4 pagesDrug Round - DigoxinErvinaDamayantiNo ratings yet
- Urinary CathetersDocument5 pagesUrinary CathetersJyoti Pariyar100% (1)
- Echo Pro Echocardiography Table: Operation ManualDocument12 pagesEcho Pro Echocardiography Table: Operation ManualCasey FriendNo ratings yet
- Webinar ReflectionDocument5 pagesWebinar ReflectionShantell NogueraNo ratings yet
- Soal Bahasa InggrisDocument5 pagesSoal Bahasa InggrisBintang MareetaNo ratings yet
- Kaufmann PlenaryDocument44 pagesKaufmann Plenaryapi-216587414No ratings yet
- Cardiology QuestionDocument63 pagesCardiology QuestionRazi Baik100% (1)
- Pediatric SIRSDocument3 pagesPediatric SIRSlalee704No ratings yet
- Aggrement PharmacyDocument2 pagesAggrement PharmacyVIKAS PANERINo ratings yet
- Crutch-WalkingDocument2 pagesCrutch-WalkingMac Cristian A. CaraganNo ratings yet