You might also like
- Diabetes HandbookDocument198 pagesDiabetes HandbookKeerthana SivarasaNo ratings yet
- Secrets of The SiddhasDocument1 pageSecrets of The SiddhasChiranth ChandNo ratings yet
- LMCC II Compilation Most RecentDocument118 pagesLMCC II Compilation Most RecentEmad Mergan100% (4)
- Handbook of NefrologyDocument244 pagesHandbook of NefrologyPopoviciu Florin MirceaNo ratings yet
- Oet Writing TipsDocument27 pagesOet Writing Tipsbjlk96% (47)
- Guidelines Microbiology Lab ProceduresDocument61 pagesGuidelines Microbiology Lab ProceduresSadao MatsumotoNo ratings yet
- Pedia Disorders Upgraded For Lnu CaDocument6 pagesPedia Disorders Upgraded For Lnu Cashirlenedel cariñoNo ratings yet
- Main 1Document4 pagesMain 1Raya KurniawanNo ratings yet
- Mercado, Marcela - 2020Document9 pagesMercado, Marcela - 2020Omar Cucho GamboaNo ratings yet
- 202 FullDocument4 pages202 FullDesi Suryani DewiNo ratings yet
- 12 Dengue Seroprevalence ComparisonDocument4 pages12 Dengue Seroprevalence ComparisonYipno Wanhar El MawardiNo ratings yet
- Utility of Serological Tests in The Era of Molecular Testing For Diagnosis of Human Brucellosis in Endemic Area With Limited ResourcesDocument4 pagesUtility of Serological Tests in The Era of Molecular Testing For Diagnosis of Human Brucellosis in Endemic Area With Limited ResourcesMiguel Pinedo TrujilloNo ratings yet
- Genexpert - On Body Fluid SpecimensDocument4 pagesGenexpert - On Body Fluid Specimensramo G.No ratings yet
- Jurnal Kulkel HemDocument5 pagesJurnal Kulkel HemAnonymous PrskyT0co6No ratings yet
- JCM 43 8 4194-4196 2005Document3 pagesJCM 43 8 4194-4196 2005Sumesh ShresthaNo ratings yet
- Na 2016Document5 pagesNa 2016abdullahkhilji.nitsNo ratings yet
- Weil-Felix Test in Diagnosis of ScrubDocument3 pagesWeil-Felix Test in Diagnosis of ScrubvyasakandarpNo ratings yet
- TJI-58070 (0) Tam Metin-Revizyon GerçekleştirilmişDocument10 pagesTJI-58070 (0) Tam Metin-Revizyon GerçekleştirilmişcerraheminNo ratings yet
- Msat - A Screening Test For Leptospirosis - Article 8Document3 pagesMsat - A Screening Test For Leptospirosis - Article 8Krishna KumarNo ratings yet
- Understanding Antigen Tests and Results ENG FinalDocument4 pagesUnderstanding Antigen Tests and Results ENG FinalAna CatarinaNo ratings yet
- 4 KNDocument25 pages4 KNMohammad Yusuf AlamudiNo ratings yet
- Mm7019a3 HDocument5 pagesMm7019a3 HShuvo H AhmedNo ratings yet
- Becker-2021-Exploring Beyond Clinical RoutineDocument12 pagesBecker-2021-Exploring Beyond Clinical RoutineNick FloresNo ratings yet
- Performance Verification of Anti-Sars-Cov-2-Specific Antibody Detection by Using Four Chemiluminescence Immunoassay SystemsDocument6 pagesPerformance Verification of Anti-Sars-Cov-2-Specific Antibody Detection by Using Four Chemiluminescence Immunoassay SystemsadnanNo ratings yet
- Bmri2016 8905675Document9 pagesBmri2016 8905675helderjamsNo ratings yet
- Serum Iga, Igm, and Igg Responses in Covid-19: Cellular & Molecular ImmunologyDocument3 pagesSerum Iga, Igm, and Igg Responses in Covid-19: Cellular & Molecular ImmunologynpidasNo ratings yet
- Comparison of Real-Time Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) and Igm-Igg Antibody Test For The Diagnosis of Sars-Cov-2 InfectionDocument18 pagesComparison of Real-Time Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) and Igm-Igg Antibody Test For The Diagnosis of Sars-Cov-2 InfectionRizki AzpiNo ratings yet
- Img#Document5 pagesImg#AngelNo ratings yet
- 10 BlythDocument6 pages10 BlythAvis UnsoedNo ratings yet
- Critical AppraisalDocument20 pagesCritical AppraisalTuty NoviantyNo ratings yet
- Evaluation Serological Diagnostic Indices For Mucocutaneous Leishmaniasis: Immunofluorescence and Enzyme-Linked For Igm and Iga AntibodiesDocument6 pagesEvaluation Serological Diagnostic Indices For Mucocutaneous Leishmaniasis: Immunofluorescence and Enzyme-Linked For Igm and Iga AntibodiesnisaNo ratings yet
- Journal of Clinical Virology: SciencedirectDocument6 pagesJournal of Clinical Virology: SciencedirectVictor VargasNo ratings yet
- Laboratory Diagnosis For DengueDocument4 pagesLaboratory Diagnosis For DengueHamid RazaNo ratings yet
- Immunodiagnosis of Tuberculosis: An Update on Antibody Detection MethodsDocument5 pagesImmunodiagnosis of Tuberculosis: An Update on Antibody Detection MethodsPROFE EFRA LAGRANGENo ratings yet
- Dengue ICT NS1 PDFDocument7 pagesDengue ICT NS1 PDFAsti Rizki Arum PermanaNo ratings yet
- Significance and Value of The Widal Test in The Diagnosis of Typhoid Fever in An Endemic AreaDocument6 pagesSignificance and Value of The Widal Test in The Diagnosis of Typhoid Fever in An Endemic AreaDavide BorgesNo ratings yet
- Anti-SARS-CoV-2 IgG Antibody Response Among Indian COVID-19 PatientsDocument6 pagesAnti-SARS-CoV-2 IgG Antibody Response Among Indian COVID-19 PatientsdhairyasheelNo ratings yet
- Avb 2005074010051Document8 pagesAvb 2005074010051Saray CorredorNo ratings yet
- Pooling of Samples For Sars-Cov-2 Detection Using A Rapid Antigen TestDocument5 pagesPooling of Samples For Sars-Cov-2 Detection Using A Rapid Antigen TestErickson OngNo ratings yet
- Basic Problems of Serological Laboratory DiagnosisDocument37 pagesBasic Problems of Serological Laboratory DiagnosisSuzan MatarNo ratings yet
- (IJCST-V4I4P22) : Elena Trajkovska-Dokic, Snezana Stojkovska, Milena Petrovska, Nikola PanovskiDocument4 pages(IJCST-V4I4P22) : Elena Trajkovska-Dokic, Snezana Stojkovska, Milena Petrovska, Nikola PanovskiEighthSenseGroupNo ratings yet
- Detection of Typhoid CarriersDocument6 pagesDetection of Typhoid CarriersClarestaNo ratings yet
- Comparison of The HIV 1 Specific Immunoglobulin GDocument5 pagesComparison of The HIV 1 Specific Immunoglobulin GAlex MorwabeNo ratings yet
- Simon 2004Document12 pagesSimon 2004mr_curiousityNo ratings yet
- Clinical Microbiology Newsletter: Genexpert Testing: Applications For Clinical Microbiology, Part IDocument5 pagesClinical Microbiology Newsletter: Genexpert Testing: Applications For Clinical Microbiology, Part ImagicianchemistNo ratings yet
- Serum Procalcitonin and C-Reactive Protein Levels As Markers of Bacterial Infection: A Systematic Review and Meta-AnalysisDocument12 pagesSerum Procalcitonin and C-Reactive Protein Levels As Markers of Bacterial Infection: A Systematic Review and Meta-AnalysissyahputriNo ratings yet
- Eurosurv 27 42 5Document13 pagesEurosurv 27 42 5Eben Leonel Albano MaiopueNo ratings yet
- Usefulness of Centor Score To Diagnosis of Group A Streptococcal Pharyngitis and Decision Making of Antibiotics UseDocument7 pagesUsefulness of Centor Score To Diagnosis of Group A Streptococcal Pharyngitis and Decision Making of Antibiotics UseAgus karsetiyonoNo ratings yet
- Rapid Diagnostic Tests Versus RT-PCR For Ebola Virus Infections: Systematic Review and Meta-AnalysisDocument24 pagesRapid Diagnostic Tests Versus RT-PCR For Ebola Virus Infections: Systematic Review and Meta-Analysissri wahyuniNo ratings yet
- Carraro 2013 RSBMTV 46 N 2 P 161Document5 pagesCarraro 2013 RSBMTV 46 N 2 P 161Emerson CarraroNo ratings yet
- Diagnostic Value of Serological Tests (IgA, IgG, IgM)Document4 pagesDiagnostic Value of Serological Tests (IgA, IgG, IgM)Gustomo PanantroNo ratings yet
- Anti-C1q Antibodies: Association With Nephritis and Disease Activity in Systemic Lupus ErythematosusDocument5 pagesAnti-C1q Antibodies: Association With Nephritis and Disease Activity in Systemic Lupus ErythematosusAlisNo ratings yet
- An Early Evaluation On The Usefulness of NS1 Antigen-Capture ELISA Versus IGM ELISA TEST For The Diagnosis of Acute Dengue InfectionDocument10 pagesAn Early Evaluation On The Usefulness of NS1 Antigen-Capture ELISA Versus IGM ELISA TEST For The Diagnosis of Acute Dengue Infectionkurniawan naryoNo ratings yet
- Volume Incidence Immunofluorescence Patterns Specific Autoantibodies 3183allasp1Document9 pagesVolume Incidence Immunofluorescence Patterns Specific Autoantibodies 3183allasp1osnolaromero4No ratings yet
- LeptospirosisDocument8 pagesLeptospirosisSanda Puspa RiniNo ratings yet
- Immunological Tests Essential and Supportive Tools in The Fight Against COVID-19Document62 pagesImmunological Tests Essential and Supportive Tools in The Fight Against COVID-19Gaspar PonceNo ratings yet
- Sepsis 2019Document12 pagesSepsis 2019EviNo ratings yet
- Prevalence of Mec A Gene Positive Coagulase Negative StaphyloDocument6 pagesPrevalence of Mec A Gene Positive Coagulase Negative Staphylosuresh151971No ratings yet
- 1-s2.0-S2212553112000908-mainDocument5 pages1-s2.0-S2212553112000908-mainbiopluslabo1No ratings yet
- Aqac126 303Document2 pagesAqac126 303Starix UkrNo ratings yet
- Fungi: Galactomannan and 1,3-β - Glucan Testing for the Diagnosis of Invasive AspergillosisDocument8 pagesFungi: Galactomannan and 1,3-β - Glucan Testing for the Diagnosis of Invasive AspergillosisntnquynhproNo ratings yet
- India CoulterDocument6 pagesIndia CoulterzainabNo ratings yet
- Sars-Cov-2 Seroconversion in Humans: A Detailed Protocol For A Serological Assay, Antigen Production, and Test SetupDocument15 pagesSars-Cov-2 Seroconversion in Humans: A Detailed Protocol For A Serological Assay, Antigen Production, and Test SetupAKNTAI002No ratings yet
- 7916 24362 1 PBDocument5 pages7916 24362 1 PBAchmad DainuriNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Rapid On-site Evaluation (ROSE): A Practical GuideFrom EverandRapid On-site Evaluation (ROSE): A Practical GuideGuoping CaiNo ratings yet
- LancetID Piafrancoetal Human Brucellosis 2007Document12 pagesLancetID Piafrancoetal Human Brucellosis 2007Abby Pérez Sa.No ratings yet
- Brucellosis - Review On The Recent Trends in Pathogenicity and Laboratory DiagnosisDocument8 pagesBrucellosis - Review On The Recent Trends in Pathogenicity and Laboratory DiagnosisJoshua SmithNo ratings yet
- Pistopoiitiko ThanatouDocument2 pagesPistopoiitiko ThanatouJoshua SmithNo ratings yet
- 1Document8 pages1Joshua SmithNo ratings yet
- Clinical Approach To Isolated Splenomegaly: M M, P M, R KDocument5 pagesClinical Approach To Isolated Splenomegaly: M M, P M, R KlilisNo ratings yet
- Proses TGL 29Document12 pagesProses TGL 29TuraaNo ratings yet
- Posterior Retroperitoneoscopic AdrenalectomyDocument14 pagesPosterior Retroperitoneoscopic AdrenalectomyShreyNo ratings yet
- (Amanda J. Jenkins) Drug Testing in Alternate BiolDocument200 pages(Amanda J. Jenkins) Drug Testing in Alternate Bioljonathan sinartaNo ratings yet
- 1 SMDocument7 pages1 SMPiaggio PIAGGIONo ratings yet
- Minor Surgical Procedures in Maxillofacial SurgeryDocument65 pagesMinor Surgical Procedures in Maxillofacial SurgerydrzibranNo ratings yet
- OrganTrade ProefschriftFrederikeAmbagtsheer PDFDocument225 pagesOrganTrade ProefschriftFrederikeAmbagtsheer PDFJanani SankarNo ratings yet
- Hypohydrotic Ectodermal DysplasiaDocument1 pageHypohydrotic Ectodermal DysplasiamaddooNo ratings yet
- ASHHNA Competency Standards For Sexual and Reproductive Health and HIV NursesDocument30 pagesASHHNA Competency Standards For Sexual and Reproductive Health and HIV NursesRNdrei dela CruzNo ratings yet
- Diagnosis-Pedrosa, Joan ADocument27 pagesDiagnosis-Pedrosa, Joan AJoan Alde PedrosaNo ratings yet
- Delivery of Evidence-Based Treatment For Multiple Anxiety Disorders in Primary Care: A Randomized Controlled TrialDocument5 pagesDelivery of Evidence-Based Treatment For Multiple Anxiety Disorders in Primary Care: A Randomized Controlled TrialRaja DarmawanNo ratings yet
- Comprehensive Edited)Document82 pagesComprehensive Edited)mikrobyo_ng_wmsuNo ratings yet
- Jurnal AnestesiDocument5 pagesJurnal AnestesiridwanNo ratings yet
- 2016 ProgramDocument30 pages2016 ProgramctyvteNo ratings yet
- Cardiovascular Risk Factors of Hypertension, Smoking and Obesity: Emerging Concerns Among Pathan and Persian Young Adults?Document5 pagesCardiovascular Risk Factors of Hypertension, Smoking and Obesity: Emerging Concerns Among Pathan and Persian Young Adults?-No ratings yet
- Post-Partum HemorrhageDocument15 pagesPost-Partum Hemorrhageapi-257029163No ratings yet
- WNHS OG PregnancyFirstTrimesterDocument60 pagesWNHS OG PregnancyFirstTrimesterBharata YudhaNo ratings yet
- Mongolian SpotsDocument9 pagesMongolian SpotsiekafzNo ratings yet
- Journal Review2Document7 pagesJournal Review2api-589685298No ratings yet
- CASE PRES PreeclampsiaDocument51 pagesCASE PRES PreeclampsiaRaiza Love Caparas-PablicoNo ratings yet
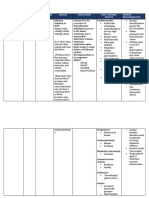
- Drug Name Brand Name Classification Dosage Indications Side/ Adverse Effects Nursing ResponsibilitiesDocument2 pagesDrug Name Brand Name Classification Dosage Indications Side/ Adverse Effects Nursing ResponsibilitiesRonald BurkeNo ratings yet
- Ayushman Bharat hospitals in BangaloreDocument163 pagesAyushman Bharat hospitals in BangaloreShreedhar KadkolNo ratings yet
- Trapdoor Effect Cause and CorrectionsDocument4 pagesTrapdoor Effect Cause and CorrectionsMarcelo BarberoNo ratings yet
- Opportunistic Mycoses: Portal of Entry: Respiratory, Mucocutaneous Infectious Particles: Conidia, MyceliaDocument4 pagesOpportunistic Mycoses: Portal of Entry: Respiratory, Mucocutaneous Infectious Particles: Conidia, MyceliaPinay YaunNo ratings yet