You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Teacher ResourcesDocument3 pagesTeacher Resourcesapi-264783804100% (1)
- Multicultural DiversityDocument14 pagesMulticultural DiversityShane Moran CanalesNo ratings yet
- On Chapter Letterhead: 2. Example - Justification LetterDocument1 pageOn Chapter Letterhead: 2. Example - Justification LetterSandie Barrie100% (2)
- List of Psychological TestsDocument28 pagesList of Psychological TestsAiraShanaAlcover100% (10)
- Grading Scale With Percentage (1091)Document1 pageGrading Scale With Percentage (1091)Bman1234No ratings yet
- BU Prospectus PDFDocument29 pagesBU Prospectus PDFPiklu ShaikhNo ratings yet
- Week20 - Unit 3 Pet ShowDocument5 pagesWeek20 - Unit 3 Pet ShowketoapimelNo ratings yet
- A4 Junior High School BrochureDocument2 pagesA4 Junior High School Brochurenurmita murdianingrumNo ratings yet
- Campus ManagentDocument694 pagesCampus ManagentEryx LetzNo ratings yet
- Cowen School Counseling PhilosophyDocument4 pagesCowen School Counseling Philosophyapi-249878488No ratings yet
- Lga 3101 PPG Module - Topic 4Document12 pagesLga 3101 PPG Module - Topic 4Anonymous HaMAMvB4No ratings yet
- Project 3 PortfolioDocument9 pagesProject 3 Portfolioapi-326369852No ratings yet
- Application For Dema-Dsi and Celma 2017-18 New May 2017Document3 pagesApplication For Dema-Dsi and Celma 2017-18 New May 2017Patrick Msase100% (1)
- Students & Writers Mostly Look For Some Questions When Coming To Paragraph Writing About Any Topic or Thing or PersonDocument2 pagesStudents & Writers Mostly Look For Some Questions When Coming To Paragraph Writing About Any Topic or Thing or PersonMst nisha AkterNo ratings yet
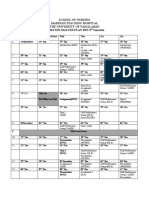
- School of Nursing Madinah Teaching Hospital The University of Faisalabad Semester Master Plan BSN 3 SemesterDocument2 pagesSchool of Nursing Madinah Teaching Hospital The University of Faisalabad Semester Master Plan BSN 3 SemesterAbeera Rajput100% (1)
- Msed Portfolio PresentationDocument7 pagesMsed Portfolio Presentationapi-365937447No ratings yet
- Two - Year Development PlanDocument21 pagesTwo - Year Development PlanTeacheer Dan100% (1)
- Letter Outreach ProgramDocument4 pagesLetter Outreach ProgramZhaidee Mambollo100% (2)
- Example 3 - Plane Areas in Rectangular Coordinates - Integral Calculus ReviewDocument5 pagesExample 3 - Plane Areas in Rectangular Coordinates - Integral Calculus ReviewRomeo VictorNo ratings yet
- ADEC - Abu Mousa Al Ashaari Private School 2016-2017Document18 pagesADEC - Abu Mousa Al Ashaari Private School 2016-2017Edarabia.comNo ratings yet
- Cot DLP Oral Com q1-2019Document1 pageCot DLP Oral Com q1-2019monette refuerzo0% (1)
- Historical Devlt Mission VissionDocument3 pagesHistorical Devlt Mission VissionGreatchen PecayoNo ratings yet
- Forming Open and Robust University Minds ActDocument14 pagesForming Open and Robust University Minds ActThe College FixNo ratings yet
- SBM Management Assessment Tool WordDocument18 pagesSBM Management Assessment Tool WordChloe Chenelle RamadlaNo ratings yet
- Outlinesofindian00mpja PDFDocument548 pagesOutlinesofindian00mpja PDFAditi BanerjeeNo ratings yet
- CalendarDocument2 pagesCalendarapi-298541847No ratings yet
- Required Examples of Compliance Evidences or - Camille IsletaDocument3 pagesRequired Examples of Compliance Evidences or - Camille IsletaJonalyn De LeonNo ratings yet
- Study Skills Syllabus 2017-2018Document3 pagesStudy Skills Syllabus 2017-2018api-366553110No ratings yet
- Requirements For Confirmation t1 Ay23 24 FroshDocument15 pagesRequirements For Confirmation t1 Ay23 24 FroshAika VillasenorNo ratings yet
- Developing Leadership Skills Among Adolescents and Young Adults A Review of Leadership ProgrammesDocument14 pagesDeveloping Leadership Skills Among Adolescents and Young Adults A Review of Leadership ProgrammesRainella SummerNo ratings yet